| PRL |
|
| Available structures |
| PDB |
Ortholog search: PDBe RCSB |
| List of PDB id codes |
|
1RW5, 2Q98, 3D48, 3EW3, 3MZG, 3N06, 3N0P, 3NCB, 3NCC, 3NCE, 3NCF, 3NPZ
|
|
|
| Identifiers |
| Aliases |
PRL, GHA1, prolactin |
| External IDs |
MGI: 97762 HomoloGene: 732 GeneCards: 5617 |
|
| Genetically Related Diseases |
| Disease Name |
References |
| mammary Paget's disease |
|
| Gene ontology |
| Molecular function |
• prolactin receptor binding
• protein binding
• hormone activity
|
| Cellular component |
• extracellular region
• intracellular
|
| Biological process |
• female pregnancy
• cellular protein metabolic process
• cell surface receptor signaling pathway
• JAK-STAT cascade involved in growth hormone signaling pathway
• lactation
• cell proliferation
• positive regulation of JAK-STAT cascade
• regulation of multicellular organism growth
|
| Sources:Amigo / QuickGO |
|
| Orthologs |
| Species |
Human |
Mouse |
| Entrez |
|
|
| Ensembl |
|
|
| UniProt |
|
|
| RefSeq (mRNA) |
|
|
| RefSeq (protein) |
|
|
NP_000939.1
NP_001157030.1
|
|
|
| Location (UCSC) |
Chr 6: 22.29 – 22.3 Mb |
Chr 13: 27.06 – 27.07 Mb |
| PubMed search |
[2] |
[3] |
| Wikidata |
| View/Edit Human |
View/Edit Mouse |
Prolactin (PRL), also known as luteotropic hormone or luteotropin, is a protein that in humans is best known for its role in enabling mammals, usually females, to produce milk. It is influential over 300 separate processes in various vertebrates.[1] Prolactin is secreted from the pituitary gland in response to eating, mating, estrogen treatment, ovulation and nursing. Prolactin is secreted in pulses in between these events. Prolactin plays an essential role in metabolism, regulation of the immune system and pancreatic development.
Discovered in non-human animals around 1930 by Oscar Riddle [2] and confirmed in humans in 1970 by Henry Friesen [3] prolactin is a peptide hormone, encoded by the PRL gene.[4]
It is associated with human milk production. In fish it is thought to be related to control of water and salt balance. Prolactin also acts in a cytokine-like manner and as an important regulator of the immune system. It has important cell cycle-related functions as a growth-, differentiating- and anti-apoptotic factor. As a growth factor, binding to cytokine-like receptors, it influences hematopoiesis, angiogenesis and is involved in the regulation of blood clotting through several pathways. The hormone acts in endocrine, autocrine and paracrine manner through the prolactin receptor and a large number of cytokine receptors.[1]
Pituitary prolactin secretion is regulated by endocrine neurons in the hypothalamus. The most important ones are the neurosecretory tuberoinfundibulum (TIDA) neurons of the arcuate nucleus that secrete dopamine (aka Prolactin Inhibitory Hormone) to act on the D2 receptors of lactotrophs, causing inhibition of prolactin secretion. Thyrotropin-releasing factor (thyrotropin-releasing hormone) has a stimulatory effect on prolactin release, however Prl is the only adenohypophyseal hormone whose principal control is inhibitory.
Several variants and forms are known per species. Many fish have variants prolactin A and prolactin B. Most vertebrates including humans also have the closely related somatolactin. In humans, three smaller (4, 16 and 22 kDa) and several larger (so called big and big-big) variants exist.[not verified in body]
Contents
- 1 Functions
- 2 Regulation
- 3 Structure and isoforms
- 4 Prolactin receptor
- 5 Diagnostic use
- 6 Units and unit conversions
- 7 Reference ranges
- 7.1 Inter-method variability
- 8 Conditions
- 8.1 Elevated levels
- 8.2 Decreased levels
- 9 See also
- 10 References
- 11 External links
Functions
Prolactin has a wide variety of effects. It stimulates the mammary glands to produce milk (lactation): increased serum concentrations of prolactin during pregnancy cause enlargement of the mammary glands and prepare for milk production, which normally starts when the levels of progesterone fall by the end of pregnancy and a suckling stimulus is present. Sometimes, newborns (males as well as females) secrete a milky substance from their nipples known as witch's milk. This is in part caused by maternal prolactin and other hormones. Prolactin plays an important role in maternal behavior.[5]
Prolactin provides the body with sexual gratification after sexual acts: The hormone counteracts the effect of dopamine, which is responsible for sexual arousal. This is thought to cause the sexual refractory period. The amount of prolactin can be an indicator for the amount of sexual satisfaction and relaxation. Unusually high amounts are suspected to be responsible for impotence and loss of libido (see hyperprolactinemia symptoms).
Elevated levels of prolactin decrease the levels of sex hormones — estrogen in women and testosterone in men.[6] The effects of mildly elevated levels of prolactin are much more variable, in women, substantially increasing or decreasing estrogen levels.
Prolactin is sometimes classified as a gonadotropin[7] although in humans it has only a weak luteotropic effect while the effect of suppressing classical gonadotropic hormones is more important.[8] Prolactin within the normal reference ranges can act as a weak gonadotropin, but at the same time suppresses GnRH secretion. The exact mechanism by which it inhibits GnRH is poorly understood. Although expression of prolactin receptors (PRL-R) have been demonstrated in rat hypothalamus, the same has not been observed in GnRH neurons.[9] Physiologic levels of prolactin in males enhance luteinizing hormone-receptors in Leydig cells, resulting in testosterone secretion, which leads to spermatogenesis.[10]
Prolactin also stimulates proliferation of oligodendrocyte precursor cells. These cells differentiate into oligodendrocytes, the cells responsible for the formation of myelin coatings on axons in the central nervous system.[11]
Other actions include contributing to pulmonary surfactant synthesis of the fetal lungs at the end of the pregnancy and immune tolerance of the fetus by the maternal organism during pregnancy. Prolactin delays hair regrowth in mice.[12] Prolactin promotes neurogenesis in maternal and fetal brains.[13][14]
Regulation
In humans, prolactin is produced at least in the anterior pituitary, decidua, myometrium, breast, lymphocytes, leukocytes and prostate.[15][16]
Pituitary PRL is controlled by the Pit-1 transcription factor that binds to the prolactin gene at several sites. Ultimately dopamine, extrapituitary PRL is controlled by a superdistal promoter and apparently unaffected by dopamine.[16] The thyrotropin-releasing hormone and the vasoactive intestinal peptide stimulate the secretion of prolactin in experimental settings, however their physiological influence is unclear. The main stimulus for prolactin secretion is suckling, the effect of which is neuronally mediated.[17] A key regulator of prolactin production is estrogens that enhance growth of prolactin-producing cells and stimulate prolactin production directly, as well as suppressing dopamine.
In decidual cells and in lymphocytes the distal promoter and thus prolactin expression is stimulated by cAMP. Responsivness to cAMP is mediated by an imperfect cAMP–responsive element and two CAAT/enhancer binding proteins (C/EBP).[16] Progesterone upregulates prolactin synthesis in the endometrium and decreases it in myometrium and breast glandular tissue.[18] Breast and other tissues may express the Pit-1 promoter in addition to the distal promoter.
Extrapituitary production of prolactin is thought to be special to humans and primates and may serve mostly tissue specific paracrine and autocrine purposes. It has been hypothesized that in vertebrates such as mice a similar tissue specific effect is achieved by a large family of prolactin-like proteins controlled by at least 26 paralogous PRL genes not present in primates.[16]
Vasoactive intestinal peptide and peptide histidine isoleucine help to regulate prolactin secretion in humans, but the functions of these hormones in birds can be quite different.[19]
Prolactin follows diurnal and ovulatory cycles. Prolactin levels peak during REM sleep and in the early morning. Many mammals experience a seasonal cycle.
During pregnancy, high circulating concentrations of estrogen and progesterone increase prolactin levels by 10- to 20-fold. Estrogen and progesterone inhibit the stimulatory effects of prolactin on milk production. The abrupt drop of estrogen and progesterone levels following delivery allow prolactin—which temporarily remains high—to induce lactation.[verification needed]
Sucking on the nipple offsets the fall in prolactin as the internal stimulus for them is removed. The sucking activates mechanoreceptors in and around the nipple. These signals are carried by nerve fibers through the spinal cord to the hypothalamus, where changes in the electrical activity of neurons that regulate the pituitary gland increase prolactin secretion. The suckling stimulus also triggers the release of oxytocin from the posterior pituitary gland, which triggers milk let-down: Prolactin controls milk production (lactogenesis) but not the milk-ejection reflex; the rise in prolactin fills the breast with milk in preparation for the next feed.
In usual circumstances, in the absence of galactorrhea, lactation ceases within one or two weeks following the end of breastfeeding.
Compared to un-mated males, fathers and expectant fathers have increased prolactin concentrations.[20]
Levels can rise after exercise, high-protein meals,[21] sexual intercourse, breast examination,[21] minor surgical procedures,[22] following epileptic seizures[23] or due to physical or emotional stress.[21][24] In a study on female volunteers under hypnosis, prolactin surges resulted from the evocation, with rage, of humiliating experiences, but not from the fantasy of nursing.[24]
Prolactin levels have also been found to rise with use of the drug MDMA (Ecstasy), leading to speculation that prolactin may have a role in the post-orgasmic state as well as decreased sexual desire.[25]
Hypersecretion is more common than hyposecretion. Hyperprolactinemia is the most frequent abnormality of the anterior pituitary tumors, termed prolactinomas. Prolactinomas may disrupt the hypothalamic-pituitary-gonadal axis as prolactin tends to suppress the secretion of GnRH from the hypothalamus and in turn decreases the secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the anterior pituitary, therefore disrupting the ovulatory cycle.[26] Such hormonal changes may manifest as amenorrhea and infertility in females as well as impotence in males. Inappropriate lactation (galactorrhoea) is another important clinical sign of prolactinomas.
Structure and isoforms
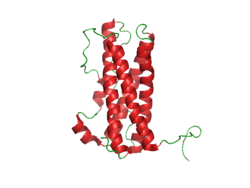
The structure of prolactin is similar to that of growth hormone and placental lactogen. The molecule is folded due to the activity of three disulfide bonds. Significant heterogeneity of the molecule has been described, thus bioassays and immunoassays can give different results due to differing glycosylation, phosphorylationsandulfation, as well as degradation. The non-glycosylated form of prolactin is the dominant form at is secreted by the pituitary gland.
The three different sizes of prolactin are:
- Little prolactin—the predominant form.[27] It has a molecular weight of appxoximately 22-kDa.[27] It is a single-chain polypeptide of 198 amino acids and is apparently the result of removal of some amino acids.
- Big prolactin—approximately 48 kDa.[27] It may be the product of interaction of several prolactin molecules. It appears to have little, if any, biological activity.[28]
- Big big prolactin—approximately 150 kDa.[27] It appears to have a low biological activity.[29]
The levels of larger ones are somewhat higher during the early postpartum period.[30]
Prolactin receptor
Main article: Prolactin receptor
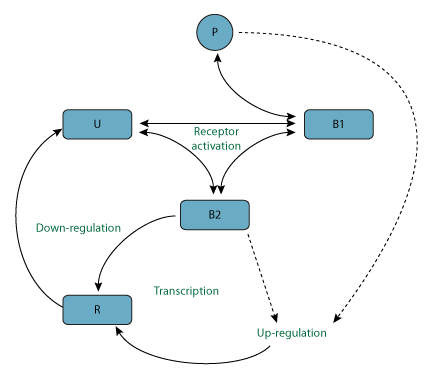
Prolactin receptors are present in the mammillary glands, ovaries, pituitary glands, heart, lung, thymus, spleen, liver, pancreas, kidney, adrenal gland, uterus, skeletal muscle, skin and areas of the central nervous system.[31] When prolactin binds to the receptor, it causes it to dimerize with another prolactin receptor. This results in the activation of Janus kinase 2, a tyrosine kinase that initiates the JAK-STAT pathway. Activation also results in the activation of mitogen-activated protein kinases and Src kinase.[31]
Human prolactin receptors are insensitive to mouse prolactin.[32]
Diagnostic use
Prolactin levels may be checked as part of a sex hormone workup, as elevated prolactin secretion can suppress the secretion of FSH and GnRH, leading to hypogonadism and sometimes causing erectile dysfunction.
Prolactin levels may be of some use in distinguishing epileptic seizures from psychogenic non-epileptic seizures. The serum prolactin level usually rises following an epileptic seizure.[33]
Units and unit conversions
The serum concentration of prolactin can be given in mass concentration (µg/L or ng/mL), molar concentration (nmol/L or pmol/L) or in international units (typically mIU/L). The current IU is calibrated against the third International Standard for Prolactin, IS 84/500.[34][35] Reference ampoules of IS 84/500 contain 2.5 µg of lyophilized human prolactin[36] and have been assigned an activity of .053 International Units.[34][35] Measurements that are calibrated against the current international standard can be converted into mass units using this ratio of grams to IUs;[37] prolactin concentrations expressed in mIU/L can be converted to µg/L by dividing by 21.2. Previous standards use other ratios.[38][39][40][41]
The first International Reference Preparation (or IRP) of human Prolactin for Immunoassay was established in 1978 (75/504 1st IRP for human Prolactin) at a time when purified human prolactin was in short supply.[37][38] Previous standards relied on prolactin from animal sources.[41] Purified human prolactin was scarce, heterogeneous, unstable and difficult to characterize. A preparation labelled 81/541 was distributed by the WHO Expert Committee on Biological Standardization without official status and given the assigned value of 50 mIU/ampoule based on an earlier collaborative study.[37][39] It was determined that this preparation behaved anomalously in certain immunoassays and was not suitable as an IS.[37]
Three different human pituitary extracts containing prolactin were subsequently obtained as candidates for an IS. These were distributed into ampoules coded 83/562, 83/573 and 84/500.[34][35][37][40] Collaborative studies involving 20 different laboratories found little difference between these three preparations. 83/562 appeared to be the most stable. This preparation was largely free of dimers and polymers of prolactin. On the basis of these investigations 83/562 was established as the Second IS for human Prolactin.[40] Once stocks of these ampoules were depleted, 84/500 was established as the Third IS for human Prolactin.[34][37]
Reference ranges
General guidelines for diagnosing prolactin excess (hyperprolactinemia) define the upper threshold of normal prolactin at 25 µg/L for women and 20 µg/L for men.[31] Similarly, guidelines for diagnosing prolactin deficiency (hypoprolactinemia) are defined as prolactin levels below 3 µg/L in women[42][43] and 5 µg/L in men.[44][45][46] However, different assays and methods for measuring prolactin are employed by different laboratories and as such the serum reference range for prolactin is often determined by the laboratory performing the measurement.[31][47] Furthermore, prolactin levels also vary factors including age,[48] sex,[48] menstrual cycle stage[48] and pregnancy.[48] The circumstances surrounding a given prolactin measurement (assay, patient condition, etc.) must therefore be considered before the measurement can be accurately interpreted.[31]
The following chart illustrates the variations seen in normal prolactin measurements across different populations. Prolactin values were obtained from specific control groups of varying sizes using the IMMULITE assay.[48]
Typical prolactin values
| Proband |
Prolactin, µg/L |
| women, follicular phase (n = 803) |
|
| women, luteal phase (n = 699) |
|
| women, mid-cycle (n = 53) |
|
| women, whole cycle (n = 1555) |
|
| women, pregnant, 1st trimester (n = 39) |
|
| women, pregnant, 2nd trimester (n = 52) |
|
| women, pregnant, 3rd trimester (n = 54) |
|
| Men, 21–30 (n = 50) |
|
| Men, 31–40 (n = 50) |
|
| Men, 41–50 (n = 50) |
|
| Men, 51–60 (n = 50) |
|
| Men, 61–70 (n = 50) |
|
Inter-method variability
The following table illustrates variability in reference ranges of serum prolactin between some commonly used assay methods (as of 2008), using a control group of healthy health care professionals (53 males, age 20–64 years, median 28 years; 97 females, age 19–59 years, median 29 years) in Essex, England:[47]
| Assay method |
Mean
Prolactin |
Lower limit
2.5th percentile |
Upper limit
97.5th percentile |
| µg/L |
mIU/L |
µg/L |
mIU/L |
µg/L |
mIU/L |
| Females |
| Centaur |
7.92 |
168 |
3.35 |
71 |
16.4 |
348 |
| Immulite |
9.25 |
196 |
3.54 |
75 |
18.7 |
396 |
| Access |
9.06 |
192 |
3.63 |
77 |
19.3 |
408 |
| AIA |
9.52[49] |
257[49] |
3.89[49] |
105[49] |
20.3[49] |
548[49] |
| Elecsys |
10.5 |
222 |
4.15 |
88 |
23.2 |
492 |
| Architect |
10.6 |
225 |
4.62 |
98 |
21.1 |
447 |
| Males |
| Access |
6.89 |
146 |
2.74 |
58 |
13.1 |
277 |
| Centaur |
7.88 |
167 |
2.97 |
63 |
12.4 |
262 |
| Immulite |
7.45 |
158 |
3.30 |
70 |
13.3 |
281 |
| AIA |
7.81[49] |
211[49] |
3.30[49] |
89[49] |
13.5[49] |
365[49] |
| Elecsys |
8.49 |
180 |
3.40 |
72 |
15.6 |
331 |
| Architect |
8.87 |
188 |
4.01 |
85 |
14.6 |
310 |
An example usage of table above is, if using the Centaur assay to estimate prolactin values in µg/L for females, the mean is 7.92 µg/L and the reference range is 3.35–16.4 µg/L.
Conditions
Elevated levels
Hyperprolactinaemia, or excess serum prolactin, is associated with hypoestrogenism, anovulatory infertility, oligomenorrhoea, amenorrhoea, unexpected lactation and loss of libido in women and erectile dysfunction and loss of libido in men.[50]
Physiological
- Coitus
- Exercise
- Lactation
- Pregnancy
- Sleep
- Stress
- Depression
|
Pharmacological
- Anesthetics
- Anticonvulsant
- Antihistamines (H2)
- Antihypertensives
- Cholinergic agonist
- Drug-induced hypersecretion
- Catecholamine depletor
- Dopamine receptor blockers
- Dopamine synthesis inhibitor
- Estrogens
- Oral contraceptives
- Oral contraceptive withdrawal
- Neuroleptics
- Antipsychotics
- Neuropeptides
- Opiates and opiate antagonists
|
Pathological
- Hypothalamic-pituitary stalk damage
- Granulomas
- Infiltrations
- Radiation
- Rathke's cyst
- Trauma
- Pituitary stalk resection
- Suprasellar surgery
- Tumors
- Craniopharyngioma
- Germinoma
- Hypothalamic metastases
- Meningioma
- Suprasellar pituitary mass extension
- Surgery
|
-
- Pituitary
- Acromegaly
- Idiopathic
- Lymphocytic hypophysitis or parasellar mass
- Macroadenoma (compressive)
- Macroprolactinemia
- Plurihumoral adenoma
- Prolactinoma
- Systemic disorders
- Chest-neurologic chest wall trauma
- Herpes Zoster
- Chronic renal failure
- Cirrhosis
- Cranial radiation
- Epileptic seizures
- Polycystic ovarian disease
- Pseudocyesis
- Chronic low levels of thyroid hormone
|
Decreased levels
Main article: Hypoprolactinemia
Hypoprolactinemia, or serum prolactin deficiency, is associated with ovarian dysfunction in women,[42][43] and arteriogenic erectile dysfunction, premature ejaculation,[44] oligozoospermia, asthenospermia, hypofunction of seminal vesicles and hypoandrogenism[45] in men. In one study, normal sperm characteristics were restored when prolactin levels were raised to normal values in hypoprolactinemic men.[46]
Hypoprolactinemia can result from hypopituitarism, excessive dopaminergic action in the tuberoinfundibular pathway and ingestion of D2 receptor agonists such as bromocriptine.
See also
- Breast-feeding
- Epileptic seizure
- Hyperprolactinaemia
- Male lactation
- Prolactin receptor
- Prolactin-releasing hormone
- Prolactinoma
- Weaning
References
- ^ a b Bole-Feysot C, Goffin V, Edery M, Binart N, Kelly PA (Jun 1998). "Prolactin (PRL) and its receptor: actions, signal transduction pathways and phenotypes observed in PRL receptor knockout mice". Endocrine Reviews 19 (3): 225–68. doi:10.1210/er.19.3.225. PMID 9626554.
- ^ Bates R, Riddle O (November 1935). "The preparation of prolactin". Journal of Pharmacolgy and Experimental Therapeutics 55 (3): 365–371.
- ^ Friesen H, Guyda H, Hardy J (Dec 1970). "The biosynthesis of human growth hormone and prolactin". The Journal of Clinical Endocrinology and Metabolism 31 (6): 611–24. doi:10.1210/jcem-31-6-611. PMID 5483096.
- ^ Evans AM, Petersen JW, Sekhon GS, DeMars R (May 1989). "Mapping of prolactin and tumor necrosis factor-beta genes on human chromosome 6p using lymphoblastoid cell deletion mutants". Somatic Cell and Molecular Genetics 15 (3): 203–13. doi:10.1007/BF01534871. PMID 2567059.
- ^ Lucas BK, Ormandy CJ, Binart N, Bridges RS, Kelly PA (Oct 1998). "Null mutation of the prolactin receptor gene produces a defect in maternal behavior". Endocrinology 139 (10): 4102–7. doi:10.1210/endo.139.10.6243. PMID 9751488.
- ^ Prolactinoma—Mayo Clinic
- ^ Hoehn K, Marieb EN (2007). Human Anatomy & Physiology. San Francisco: Pearson Benjamin Cummings. p. 605. ISBN 0-8053-5909-5.
- ^ Gonadotropins at the US National Library of Medicine Medical Subject Headings (MeSH)
- ^ Grattan DR, Jasoni CL, Liu X, Anderson GM, Herbison AE (Sep 2007). "Prolactin regulation of gonadotropin-releasing hormone neurons to suppress luteinizing hormone secretion in mice". Endocrinology 148 (9): 4344–51. doi:10.1210/en.2007-0403. PMID 17569755.
- ^ Hair WM, Gubbay O, Jabbour HN, Lincoln GA (Jul 2002). "Prolactin receptor expression in human testis and accessory tissues: localization and function". Molecular Human Reproduction 8 (7): 606–11. doi:10.1093/molehr/8.7.606. PMID 12087074.
- ^ Gregg C, Shikar V, Larsen P, Mak G, Chojnacki A, Yong VW, Weiss S (Feb 2007). "White matter plasticity and enhanced remyelination in the maternal CNS". The Journal of Neuroscience 27 (8): 1812–23. doi:10.1523/JNEUROSCI.4441-06.2007. PMID 17314279.
- ^ Craven AJ, Nixon AJ, Ashby MG, Ormandy CJ, Blazek K, Wilkins RJ, Pearson AJ (Nov 2006). "Prolactin delays hair regrowth in mice". The Journal of Endocrinology 191 (2): 415–25. doi:10.1677/joe.1.06685. PMID 17088411.
- ^ Shingo T, Gregg C, Enwere E, Fujikawa H, Hassam R, Geary C, Cross JC, Weiss S (Jan 2003). "Pregnancy-stimulated neurogenesis in the adult female forebrain mediated by prolactin". Science 299 (5603): 117–20. doi:10.1126/science.1076647. PMID 12511652.
- ^ Larsen CM, Grattan DR (Feb 2012). "Prolactin, neurogenesis, and maternal behaviors". Brain, Behavior, and Immunity 26 (2): 201–9. doi:10.1016/j.bbi.2011.07.233. PMID 21820505.
- ^ Ben-Jonathan N, Mershon JL, Allen DL, Steinmetz RW (Dec 1996). "Extrapituitary prolactin: distribution, regulation, functions, and clinical aspects". Endocrine Reviews 17 (6): 639–69. doi:10.1210/edrv-17-6-639. PMID 8969972.
- ^ a b c d Gerlo S, Davis JR, Mager DL, Kooijman R (Oct 2006). "Prolactin in man: a tale of two promoters". BioEssays 28 (10): 1051–5. doi:10.1002/bies.20468. PMC 1891148. PMID 16998840.
- ^ Norman AW, Henry HL, eds. (2014). "III. Structure, Synthesis, Secretion, and Target Cells of the Hypothalamic Releasing Hormones: E. Hypothalamic Control of Prolactin Secretion". Hormones. Academic Press. p. 66. ISBN 9780080919065.
- ^ Zinger M, McFarland M, Ben-Jonathan N (Feb 2003). "Prolactin expression and secretion by human breast glandular and adipose tissue explants". The Journal of Clinical Endocrinology and Metabolism 88 (2): 689–96. doi:10.1210/jc.2002-021255. PMID 12574200.
- ^ Kulick RS, Chaiseha Y, Kang SW, Rozenboim I, El Halawani ME (Jul 2005). "The relative importance of vasoactive intestinal peptide and peptide histidine isoleucine as physiological regulators of prolactin in the domestic turkey". General and Comparative Endocrinology 142 (3): 267–73. doi:10.1016/j.ygcen.2004.12.024. PMID 15935152.
- ^ Nelson, Randy F. (2011). An Introduction to Behavioral Endocrinology (Fourth ed.). Sunderland, Mass: Sinauer Associates Inc. p. 438. ISBN 0-87893-620-3.
- ^ a b c "Prolactin". MedLine plus. Retrieved 2014-10-24.
- ^ Melmed S, Jameson JL (2005). "333 Disorders of the Anterior Pituitary and Hypothalamus". In Jameson JN, Kasper DL, Harrison TR, Braunwald E, Fauci AS, Hauser SL, Longo DL. Harrison's principles of internal medicine (16th ed.). New York: McGraw-Hill Medical Publishing Division. ISBN 0-07-140235-7.
- ^ Mellers JD (Aug 2005). "The approach to patients with "non-epileptic seizures"". Postgraduate Medical Journal 81 (958): 498–504. doi:10.1136/pgmj.2004.029785. PMC 1743326. PMID 16085740.
- ^ a b Sobrinho LG (2003). "Prolactin, psychological stress and environment in humans: adaptation and maladaptation". Pituitary 6 (1): 35–9. doi:10.1023/A:1026229810876. PMID 14674722.
- ^ "Ecstasy (MDMA) mimics the post-orgasmic state: impairment of sexual drive and function during acute MDMA-effects may be due to increased prolactin secretion.". PubMed. Retrieved 11 August 2015.
- ^ "Etiology, diagnosis, and treatment of secondary amenorrhea". Retrieved 7 November 2013.
- ^ a b c d Sabharwal P, Glaser R, Lafuse W, Varma S, Liu Q, Arkins S, Kooijman R, Kutz L, Kelley KW, Malarkey WB (Aug 1992). "Prolactin synthesized and secreted by human peripheral blood mononuclear cells: an autocrine growth factor for lymphoproliferation". Proceedings of the National Academy of Sciences of the United States of America 89 (16): 7713–6. doi:10.1073/pnas.89.16.7713. PMC 49781. PMID 1502189. , in turn citing: Kiefer KA, Malarkey WB (Jan 1978). "Size heterogeneity of human prolactin in CSF and serum: experimental conditions that alter gel filtration patterns". The Journal of Clinical Endocrinology and Metabolism 46 (1): 119–24. doi:10.1210/jcem-46-1-119. PMID 752015.
- ^ Garnier PE, Aubert ML, Kaplan SL, Grumbach MM (Dec 1978). "Heterogeneity of pituitary and plasma prolactin in man: decreased affinity of "Big" prolactin in a radioreceptor assay and evidence for its secretion". The Journal of Clinical Endocrinology and Metabolism 47 (6): 1273–81. doi:10.1210/jcem-47-6-1273. PMID 263349.
- ^ Leite V, Cosby H, Sobrinho LG, Fresnoza MA, Santos MA, Friesen HG (Oct 1992). "Characterization of big, big prolactin in patients with hyperprolactinaemia". Clinical Endocrinology 37 (4): 365–72. doi:10.1111/j.1365-2265.1992.tb02340.x. PMID 1483294.
- ^ Kamel MA, Neulen J, Sayed GH, Salem HT, Breckwoldt M (Sep 1993). "Heterogeneity of human prolactin levels in serum during the early postpartum period". Gynecological Endocrinology 7 (3): 173–7. doi:10.3109/09513599309152499. PMID 8291454.
- ^ a b c d e Mancini T, Casanueva FF, Giustina A (Mar 2008). "Hyperprolactinemia and prolactinomas". Endocrinology and Metabolism Clinics of North America 37 (1): 67–99, viii. doi:10.1016/j.ecl.2007.10.013. PMID 18226731.
- ^ Utama FE, LeBaron MJ, Neilson LM, Sultan AS, Parlow AF, Wagner KU, Rui H (Mar 2006). "Human prolactin receptors are insensitive to mouse prolactin: implications for xenotransplant modeling of human breast cancer in mice". The Journal of Endocrinology 188 (3): 589–601. doi:10.1677/joe.1.06560. PMID 16522738.
- ^ Banerjee S, Paul P, Talib VJ (Aug 2004). "Serum prolactin in seizure disorders". Indian Pediatrics 41 (8): 827–31. PMID 15347871.
- ^ a b c d Schulster D, Gaines Das RE, Jeffcoate SL (Apr 1989). "International Standards for human prolactin: calibration by international collaborative study". The Journal of Endocrinology 121 (1): 157–66. doi:10.1677/joe.0.1210157. PMID 2715755.
- ^ a b c "WHO Expert Committee on Biological Standardization" (PDF). Thirty-ninth Report, WHO Technical Report Series. World Health Organization. 1989. Retrieved 2009-06-03.
86.1520, WHO/BS documents: 86.1520 Add 1, 88.1596
- ^ "WHO International Standard, Prolactin, Human. NIBSC code: 84/500, Instructions for use" (PDF). WHO International Standard, Prolactin, Human. NIBSC code: 84/500, Instructions for use. NIBSC / Health Protection Agency. 1989. Retrieved 2011-03-21.
- ^ a b c d e f Canadian Society of Clinical Chemists (Dec 1992). "Canadian Society of Clinical Chemists position paper: standardization of selected polypeptide hormone measurements". Clinical Biochemistry 25 (6): 415–24. doi:10.1016/0009-9120(92)90030-V. PMID 1477965.
- ^ a b Gaines Das RE, Cotes PM (Jan 1979). "International Reference Preparation of human prolactin for immunoassay: definition of the International Unit, report of a collaborative study and comparison of estimates of human prolactin made in various laboratories". The Journal of Endocrinology 80 (1): 157–68. doi:10.1677/joe.0.0800157. PMID 429949.
- ^ a b "WHO Expert Committee on Biological Standardization" (PDF). Thirty-fifth Report, WHO Technical Report Series. World Health Organization. 1985. Retrieved 2011-03-21.
- ^ a b c "WHO Expert Committee on Biological Standardization" (PDF). Thirty-seventh Report, WHO Technical Report Series. World Health Organization. 1987. Retrieved 2011-03-21.
- ^ a b Bangham DR, Mussett MV, Stack-Dunne MP (1963). "THE SECOND INTERNATIONAL STANDARD FOR PROLACTIN". Bulletin of the World Health Organization 29 (6): 721–8. PMC 2555104. PMID 14107744.
- ^ a b Kauppila A, Martikainen H, Puistola U, Reinilä M, Rönnberg L (Mar 1988). "Hypoprolactinemia and ovarian function". Fertility and Sterility 49 (3): 437–41. PMID 3342895.
- ^ a b Schwärzler P, Untergasser G, Hermann M, Dirnhofer S, Abendstein B, Berger P (Oct 1997). "Prolactin gene expression and prolactin protein in premenopausal and postmenopausal human ovaries". Fertility and Sterility 68 (4): 696–701. doi:10.1016/S0015-0282(97)00320-8. PMID 9341613.
- ^ a b Corona G, Mannucci E, Jannini EA, Lotti F, Ricca V, Monami M, Boddi V, Bandini E, Balercia G, Forti G, Maggi M (May 2009). "Hypoprolactinemia: a new clinical syndrome in patients with sexual dysfunction". The Journal of Sexual Medicine 6 (5): 1457–66. doi:10.1111/j.1743-6109.2008.01206.x. PMID 19210705.
- ^ a b Gonzales GF, Velasquez G, Garcia-Hjarles M (1989). "Hypoprolactinemia as related to seminal quality and serum testosterone". Archives of Andrology 23 (3): 259–65. doi:10.3109/01485018908986849. PMID 2619414.
- ^ a b Ufearo CS, Orisakwe OE (Sep 1995). "Restoration of normal sperm characteristics in hypoprolactinemic infertile men treated with metoclopramide and exogenous human prolactin". Clinical Pharmacology and Therapeutics 58 (3): 354–9. doi:10.1016/0009-9236(95)90253-8. PMID 7554710.
- ^ a b Table 2 in Beltran L, Fahie-Wilson MN, McKenna TJ, Kavanagh L, Smith TP (Oct 2008). "Serum total prolactin and monomeric prolactin reference intervals determined by precipitation with polyethylene glycol: evaluation and validation on common immunoassay platforms". Clinical Chemistry 54 (10): 1673–81. doi:10.1373/clinchem.2008.105312. PMID 18719199.
- ^ a b c d e Prolaktin at medical.siemens.com—reference ranges as determined from the IMMULITE assay method
- ^ a b c d e f g h i j k l The AIA essay values are also from Table 2 in Beltran 2008, like the other values, but it uses a different conversion factor of 27.0 mIU/L per µg/L, taken from the second international standard, IS 83/562).
- ^ Melmed S, Kleinberg D 2008 Anterior pituitary. 1n: Kronenberg HM, Melmed S, Polonsky KS, Larsen PR, eds. Willams textbook of endocrinology. 11th ed. Philadelphia: Saunders Elsevier; 185-261
External links
- Pathophysiology of Endocrine System—Prolactin at colostate.edu
- MedlinePlus Encyclopedia Prolactin
- Prolactin - Lab Tests Online
- med/1098 at eMedicine—"Hyperprolactinemia"
- med/1914 at eMedicine—"Prolactin Deficiency"
- [4] - "Endocrine Society Guidelines"
|
Hormones
|
|
Endocrine
glands |
|
Hypothalamic-
pituitary
|
|
Hypothalamus
|
- GnRH
- TRH
- Dopamine
- CRH
- GHRH
- Somatostatin (GHIH)
- MCH
|
|
|
Posterior pituitary
|
|
|
|
Anterior pituitary
|
- FSH
- LH
- TSH
- Prolactin
- POMC
- CLIP
- ACTH
- MSH
- Endorphins
- Lipotropin
- GH
|
|
|
|
Adrenal axis
|
- Adrenal cortex
- aldosterone
- cortisol
- cortisone
- DHEA
- testosterone
- Adrenal medulla
- epinephrine
- norepinephrine
|
|
|
Thyroid
|
- Thyroid hormone
- Calcitonin
- Thyroid axis
|
|
|
Parathyroid
|
|
|
|
|
Gonadal axis
|
|
Testis
|
|
|
|
Ovary
|
- estradiol
- progesterone
- activin and inhibin
- relaxin (pregnancy)
|
|
|
Placenta
|
- hCG
- HPL
- estrogen
- progesterone
|
|
|
|
Pancreas
|
- glucagon
- insulin
- amylin
- somatostatin
- pancreatic polypeptide
|
|
|
Pineal gland
|
- melatonin
- N,N-dimethyltryptamine
- 5-methoxy-N,N-dimethyltryptamine
|
|
|
| Other |
|
Thymus
|
- Thymosins
- Thymosin α1
- Beta thymosins
- Thymopoietin
- Thymulin
|
|
|
Digestive system
|
|
Stomach
|
|
|
|
Duodenum
|
- CCK
- Incretins
- secretin
- motilin
- VIP
|
|
|
Ileum
|
- enteroglucagon
- peptide YY
|
|
|
Liver/other
|
- Insulin-like growth factor
|
|
|
|
Adipose tissue
|
- leptin
- adiponectin
- resistin
|
|
|
Skeleton
|
|
|
|
Kidney
|
- JGA (renin)
- peritubular cells
- calcitriol
- prostaglandin
|
|
|
Heart
|
|
|
|
|
Amyloidosis (E85, 277.3)
|
|
| Common amyloid forming proteins |
- AA
- ATTR
- Aβ2M
- AL
- Aβ/APP
- AIAPP
- ACal
- APro
- AANF
- ACys
- ABri
|
|
| Systemic amyloidosis |
- AL amyloidosis
- AA amyloidosis
- Aβ2M/Haemodialysis-associated
- AGel/Finnish type
- AA/Familial Mediterranean fever
- ATTR/Transthyretin-related hereditary
|
|
| Organ-limited amyloidosis |
|
Heart
|
AANF/Isolated atrial
|
|
|
Brain
|
- Familial amyloid neuropathy
- ACys+ABri/Cerebral amyloid angiopathy
- Aβ/Alzheimer's disease
|
|
|
Kidney
|
- AApoA1+AFib+ALys/Familial renal
|
|
|
Cutaneous
|
- Primary cutaneous amyloidosis
- Amyloid purpura
|
|
|
Endocrine
|
- Thyroid
- ACal/Medullary thyroid cancer
- Pituitary
- APro/Prolactinoma
- Pancreas
- AIAPP/Insulinoma
- AIAPP/Diabetes mellitus type 2
|
|
|
|
Protein and peptide receptor modulators
|
|
| Adiponectin |
|
AdipoR1
|
- Agonists: Peptide: Adiponectin
- ADP-355
- ADP-399; Non-peptide: AdipoRon
- (–)-Arctigenin
- Arctiin
- Gramine
- Matairesinol
- Antagonists: Peptide: ADP-400
|
|
|
AdipoR2
|
- Agonists: Peptide: Adiponectin
- ADP-355
- ADP-399; Non-peptide: AdipoRon
- Deoxyschizandrin
- Parthenolide
- Syringing
- Taxifoliol
- Antagonists: Peptide: ADP-400
|
|
|
| Angiotensin |
- Agonists: Angiotensin II
- Angiotensin III
- Angiotensin IV
- Saralasin
- Antagonists: Abitesartan
- Azilsartan
- Azilsartan medoxomil
- Candesartan
- Elisartan
- Embusartan
- Eprosartan
- EXP-3174
- Fimasartan
- Forasartan
- Irbesartan
- Losartan
- Milfasartan
- Olmesartan
- Olmesartan medoxomil
- PD123319
- Pomisartan
- Pratosartan
- Ripisartan
- Saprisartan
- Sparsentan
- Tasosartan
- Telmisartan
- Valsartan
- Zolasartan
- ACE inhibitors: Alacepril
- Benazepril
- Captopril
- Cilazapril
- Delapril
- Enalapril
- Enalaprilat
- Fosinopril
- Gemopatrilat
- Imidapril
- Lisinopril
- Moexipril
- Omapatrilat
- Perindopril
- Quinapril
- Quinaprilat
- Ramipril
- Rentiapril
- Rescinnamine
- Spirapril
- Spiraprilat
- Temocapril
- Trandolapril
- Zofenopril
- Zofenoprilat
- Renin inhibitors: Aliskiren
- Ciprokiren
- Ditekiren
- Enalkiren
- Pepstatin
- Remikiren
- Terlakiren
- Zankiren
- Propeptides: Angiotensinogen
- Angiotensin I
|
|
| Bradykinin |
- Agonists: Bradykinin
- Kallidin
- Antagonists: FR-173657
- Icatibant
- LF22-0542
|
|
| CGRP |
- Agonists: Amylin
- CGRP
- Pramlintide
- Antagonists: BI 44370 TA
- BMS-927711
- CGRP (8-37)
- MK-3207
- Olcegepant
- Rimegepant
- SB-268262
- Telcagepant
- Ubrogepant
|
|
| Cholecystokinin |
|
CCKA
|
- Agonists: Cholecystokinin
- CCK-4
- Antagonists: Amiglumide
- Asperlicin
- Devazepide
- Dexloxiglumide
- Lintitript
- Lorglumide
- Loxiglumide
- Pranazepide
- Proglumide
- Tarazepide
- Tomoglumide
|
|
|
CCKB
|
- Agonists: Cholecystokinin
- CCK-4
- Gastrin
- Antagonists: CI-988 (PD-134308)
- Itriglumide
- L-365,360
- Netazepide
- Proglumide
- Spiroglumide
|
|
|
Unsorted
|
- Antagonists: Nastorazepide
|
|
|
| CRH |
|
CRF1
|
- Agonists: Cortagine
- Corticorelin
- Corticotropin releasing hormone
- Sauvagine
- Stressin I
- Urocortin
- Antagonists: Antalarmin
- Astressin-B
- CP-154,526
- Emicerfont
- Hypericin
- LWH-234
- NBI-27914
- Pexacerfont
- R-121919
- TS-041
- Verucerfont
|
|
|
CRF2
|
- Agonists: Corticorelin
- Corticotropin releasing hormone
- Sauvagine
- Urocortin
|
|
|
| Cytokine |
See here instead.
|
|
| Endothelin |
- Agonists: Endothelin 1
- Endothelin 2
- Endothelin 3
- IRL-1620
- Antagonists: A-192621
- ACT-132577
- Ambrisentan
- Atrasentan
- Avosentan
- Bosentan
- BQ-123
- BQ-788
- Clazosentan
- Darusentan
- Edonentan
- Enrasentan
- Fandosentan
- Feloprentan
- Macitentan
- Nebentan
- Sitaxentan
- Sparsentan
- Tezosentan
- Zibotentan
|
|
| Galanin |
|
GAL1
|
- Agonists: Galanin
- Galanin (1-15)
- Galanin-like peptide
- Galmic
- Galnon
- Antagonists: C7
- Dithiepine-1,1,4,4-tetroxide
- Galantide (M15)
- M32
- M35
- M40
- SCH-202596
|
|
|
GAL2
|
- Agonists: Galanin
- Galanin (1-15)
- Galanin (2-11)
- Galanin-like peptide
- Galmic
- Galnon
- J18
- Antagonists: C7
- Galantide (M15)
- M32
- M35
- M40
- M871
|
|
|
GAL3
|
- Agonists: Galanin
- Galanin (1-15)
- Galmic
- Galnon
- Antagonists: C7
- Galantide (M15)
- GalR3ant
- HT-2157
- M32
- M35
- M40
- SNAP-37889
- SNAP-398299
|
|
|
| Ghrelin/GHS |
- Agonists: Peptide: Alexamorelin
- Cortistatin-14
- Examorelin (hexarelin)
- Ghrelin
- GHRP-1
- GHRP-3
- GHRP-4
- GHRP-5
- GHRP-6
- Ipamorelin
- Lenomorelin
- Pralmorelin (GHRP-2)
- Relamorelin
- Tabimorelin
- Ulimorelin; Non-peptide: Adenosine
- Anamorelin
- Capromorelin
- CP-464709
- Ibutamoren (MK-677)
- L-692,585
- Macimorelin
- SM-130686; Unsorted: LY-426410
- LY-444711
- Antagonists: A-778193
- Cortistatin-8
- (D-Lys³)-GHRP-6
- JMV2959
- YIL-781
- Binding proteins: Growth hormone-binding protein
|
|
| GH |
- Agonists: Bovine somatotropin
- Efpegsomatropin
- Growth hormone
- Human placental lactogen
- MOD-4023
- Somagrebove
- Somapacitan
- Somatosalm
- Somatotropin
- Somatropin pegol
- Somatrem
- Sometribove
- Somavaratan
- Somavubove
- Somidobove
- Antagonists: G120K-hGH
- Pegvisomant
|
|
| GHRH |
- Agonists: Peptide: CJC-1295
- Dumorelin
- GHRH
- Modified GRF (1-29)
- Rismorelin
- Sermorelin
- Somatorelin
- Tesamorelin
|
|
| GLP |
|
GLP-1
|
- Agonists: Albiglutide
- Dulaglutide
- Efpeglenatide
- Exenatide
- GLP-1
- Langlenatide
- Liraglutide
- Lixisenatide
- Oxyntomodulin
- Semaglutide
- Taspoglutide
|
|
|
GLP-2
|
- Agonists: Elsiglutide
- GLP-2
- Teduglutide
|
|
|
Others
|
- Propeptides: Preproglucagon
- Proglucagon
|
|
|
| Glucagon |
- Agonists: Glucagon
- Oxyntomodulin
- Antagonists: L-168,049
- LGD-6972
- Propeptides: Preproglucagon
- Proglucagon
|
|
| GnRH |
- Agonists: Peptide: Avorelin
- Buserelin
- Deslorelin
- Gonadorelin
- GnRH (LHRH)
- Goserelin
- Histrelin
- Leuprorelin
- Lutrelin
- Nafarelin
- Peforelin
- Triptorelin
- Zoptarelin doxorubicin
- Antagonists: Peptide: Abarelix
- Acyline
- Cetrorelix
- Degarelix
- Detirelix
- Ganirelix
- Iturelix
- Ozarelix
- Prazarelix
- Ramorelix
- Teverelix (antarelix); Non-peptide: ASP-1707
- Elagolix
- KLH-2109
- Relugolix
- Sufugolix
|
|
| Gonadotropin |
|
LH/CG
|
- Agonists: Choriogonadotropin alfa
- Human chorionic gonadotropin
- Luteinizing hormone
- Lutropin alfa
- Menotropin (human menopausal gonadotropin)
|
|
|
FSH
|
- Agonists: Corifollitropin alfa
- Follicle-stimulating hormone
- Follitropin alfa
- Follitropin beta
- Menotropin (human menopausal gonadotropin)
- Urofollitropin
- Varfollitropin alfa
|
|
|
| Growth factor |
See here instead.
|
|
| Insulin |
- Agonists: Insulin-like growth factor 1
- Insulin-like growth factor 2
- Insulin
- Insulin aspart
- Insulin degludec
- Insulin detemir
- Insulin glargine
- Insulin glulisine
- Insulin lispro
- Mecasermin
- Mecasermin rinfabate
- Antagonists: BMS-754807
- S661
- S961
- Kinase inhibitors: Linsitinib
|
|
| Kisspeptin |
- Agonists: Kisspeptin
- Kisspeptin-10
- Antagonists: Kisspeptin-234
|
|
| Leptin |
- Agonists: Leptin
- Metreleptin
|
|
| MCH |
|
MCH1
|
- Agonists: Melanin concentrating hormone
- Antagonists: ATC-0065
- ATC-0175
- GW-803430
- NGD-4715
- SNAP-7941
- SNAP-94847
|
|
|
MCH2
|
- Agonists: Melanin concentrating hormone
|
|
|
| Melanocortin |
|
|
| Neuropeptide FF |
- Agonists: Neuropeptide AF
- Neuropeptide FF
- Neuropeptide SF (RFRP-1)
- Neuropeptide VF (RFRP-3)
- Antagonists: BIBP-3226
- RF9
|
|
| Neuropeptide S |
- Antagonists: ML-154
- SHA-68
|
|
| Neuropeptide Y |
|
Y1
|
- Agonists: Neuropeptide Y
- Peptide YY
- Antagonists: BIBO-3304
- BIBP-3226
- BVD-10
- GR-231118
- PD-160170
|
|
|
Y2
|
- Agonists: 2-Thiouridine 5'-triphosphate
- Neuropeptide Y
- Neuropeptide Y (13-36)
- Peptide YY
- Peptide YY (3-36)
- Antagonists: BIIE-0246
- JNJ-5207787
- SF-11
|
|
|
Y4
|
- Agonists: GR-231118
- Neuropeptide Y
- Pancreatic polypeptide
- Peptide YY
|
|
|
Y5
|
- Agonists: BWX-46
- Neuropeptide Y
- Peptide YY
- Antagonists: CGP-71683
- FMS-586
- L-152,804
- Lu AA-33810
- MK-0557
- NTNCB
- Velneperit (S-2367)
|
|
|
| Neurotensin |
|
NTS1
|
- Agonists: Neurotensin
- Neuromedin N
- Antagonists: Meclinertant
- SR-142948
|
|
|
NTS2
|
- Antagonists: Levocabastine
- SR-142948
|
|
|
| Opioid |
See here instead.
|
|
| Orexin |
|
OX1
|
- Antagonists: ACT-335827
- ACT-462206
- Almorexant
- Filorexant
- Lemborexant
- SB-334867
- SB-408124
- SB-649868
- Suvorexant
- TCS-1102
|
|
|
OX2
|
- Agonists: Orexin (A, B)
- SB-668875
- Antagonists: ACT-335827
- ACT-462206
- Almorexant
- EMPA
- Filorexant
- JNJ-10397049
- MIN-202 (JNJ-42847922)
- Lemborexant
- MK-1064
- SB-649868
- Suvorexant
- TCS-1102
- TCS-OX2-29
|
|
|
| Oxytocin |
|
|
| Prolactin |
- Agonists: Growth hormone
- Human placental lactogen
- Prolactin
- S179D-hPRL
- Somatotropin
- Antagonists: Δ1–9-G129R-hPRL
- Δ1–14-G129R-hPRL
- G120K-hGH
- G129R-hPRL
|
|
| PTH |
- Agonists: Abaloparatide
- Parathyroid hormone
- Parathyroid hormone-related protein (PTHrP)
- Semparatide
- Teriparatide
|
|
| Relaxin |
- Agonists: Insulin-like factor 3
- Relaxin (1, 2, 3)
- Serelaxin
|
|
| Somatostatin |
- Agonists: BIM-23052
- CH-275
- Cortistatin-14
- Depreotide
- Ilatreotide
- L-803,087
- L-817,818
- Lanreotide
- NNC 26-9100
- Octreotide
- Pasireotide
- Pentetreotide
- RC-160
- Seglitide
- Somatostatin (GHIH)
- Somatostatin (1-28)
- SRIF-14
- SRIF-28
- TT-232
- Vapreotide
- Antagonists: BIM-23056
- Cyclosomatostatin
- CYN-154806
|
|
| Tachykinin |
|
NK1
|
- Antagonists: Aprepitant
- Befetupitant
- Burapitant
- Casopitant
- CI-1021
- CP-96345
- CP-99994
- CP-122721
- Dapitant
- Ezlopitant
- Figopitant
- FK-888
- Fosaprepitant
- Fosnetupitant
- GR-203040
- GW-597599
- HSP-117
- L-733,060
- L-741,671
- L-743,310
- L-758,298
- Lanepitant
- LY-306740
- Maropitant
- Netupitant
- NKP-608
- Nolpitantium besilate
- Orvepitant
- Rolapitant
- RP-67580
- SDZ NKT 343
- Serlopitant
- Telmapitant
- Tradipitant
- Vestipitant
- Vofopitant
|
|
|
NK2
|
- Antagonists: GR-159897
- Ibodutant
- Nepadutant
- Saredutant
|
|
|
NK3
|
- Antagonists: Osanetant
- Talnetant
|
|
|
| TRH |
- Agonists: Azetirelin
- Fertirelin
- Montirelin
- Orotirelin
- Posatirelin
- Protirelin
- Rovatirelin
- Taltirelin
- TRH (TRF)
|
|
| TSH |
- Agonists: Thyrotropin alfa
- TSH (thyrotropin)
|
|
| Vasopressin |
|
|
| VIP/PACAP |
|
VIPR1
|
- Agonists: Peptide: Bay 55-9837
- LBT-3393
- PACAP
- VIP
|
|
|
VIPR2
|
- Agonists: Peptide: LBT-3627
- PACAP
- VIP
|
|
|
PAC1
|
- Agonists: PACAP
- PACAP (1-27)
- PACAP (1-38)
- Antagonists: PACAP (6-38)
|
|
|
Unsorted
|
|
|
|
| Others |
- Adrenomedullin
- Apelin
- Bombesin
- Calcitonin
- Carnosine
- CART
- CLIP
- DSIP
- Enteroglucagon
- Formyl peptide
- GALP
- GIP
- GRP
- Integrin ligands (collagens, fibrinogen, fibronectin, laminins, ICAM-1, ICAM-2, osteopontin, VCAM-1, vitronectin)
- Kininogens
- Motilin
- Natriuretic peptides (ANP, BNP, CNP, urodilatin)
- Nesfatin-1
- Neuromedin B
- Neuromedin N
- Neuromedin S
- Neuromedin U
- Obestatin
- Osteocalcin
- Resistin
- Secretin
- Thymopoietin
- Thymosins
- Thymulin
- Urotensin-II
- VGF
|
|