WordNet
- any neuropathy of a single nerve trunk
Wikipedia preview
出典(authority):フリー百科事典『ウィキペディア(Wikipedia)』「2015/09/25 23:44:33」(JST)
wiki en
Not to be confused with Nephropathy or Neuropathology.
| Peripheral neuropathy | |
|---|---|
|
Micrograph showing a vasculitic peripheral neuropathy; plastic embedded; Toluidine blue stain
|
|
| Classification and external resources | |
| Specialty | Neurology |
| ICD-10 | G64, G90.0 |
| ICD-9-CM | 356.0, 356.8 |
| DiseasesDB | 9850 |
| MedlinePlus | 000593 |
| Patient UK | Peripheral neuropathy |
| MeSH | D010523 |
Peripheral neuropathy (PN) is damage to or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected. Common causes include systemic diseases (such as diabetes or leprosy), vitamin deficiency, medication (e.g., chemotherapy), traumatic injury, radiation therapy, excessive alcohol consumption, immune system disease or viral infection. It can also be genetic (present from birth) or idiopathic (no known cause).[1][2][3] In conventional medical usage, the word neuropathy (neuro-, "nervous system" and -pathy, "disease of")[4] without modifier usually means peripheral neuropathy. Neuropathy affecting just one nerve is called "mononeuropathy" and neuropathy involving multiple nerves in roughly the same areas on both sides of the body is called "symmetrical polyneuropathy" or simply "polyneuropathy." When two or more (typically just a few, but sometimes many) separate nerves in disparate areas of the body are affected it is called "mononeuritis multiplex," "multifocal mononeuropathy," or "multiple mononeuropathy."[1][2][3] Peripheral neuropathy may be chronic (a long term condition where symptoms begin subtly and progress slowly) or acute (sudden onset, rapid progress, and slow resolution). Acute neuropathies demand urgent diagnosis. Motor nerves (that control muscles), sensory nerves, or autonomic nerves (that control automatic functions such as heart rate, body temperature, and breathing), may be affected. More than one type of nerve may be affected at the same time. Peripheral neuropathies may be classified according to the type of nerve predominantly involved, or by the underlying cause. Where the cause is unknown it is described as idiopathic neuropathy.[1][2][3]
Neuropathy may cause painful cramps, fasciculations (fine muscle twitching), muscle loss, bone degeneration, and changes in the skin, hair, and nails. Additionally, motor neuropathy may cause impaired balance and coordination or, most commonly, muscle weakness; sensory neuropathy may cause numbness to touch and vibration, reduced position sense causing poorer coordination and balance, reduced sensitivity to temperature change and pain, spontaneous tingling or burning pain, or skin allodynia (severe pain from normally nonpainful stimuli, such as light touch); and autonomic neuropathy may produce diverse symptoms, depending on the affected glands and organs, but common symptoms are poor bladder control, abnormal blood pressure or heart rate, and reduced ability to sweat normally.[1][2][3]
Contents
- 1 Classification
- 1.1 Mononeuropathy
- 1.2 Mononeuritis multiplex
- 1.3 Polyneuropathy
- 1.4 Autonomic neuropathy
- 1.5 Neuritis
- 2 Signs and symptoms
- 3 Diagnosis
- 4 Causes
- 5 Treatment
- 6 References
- 7 Further reading
Classification
Peripheral neuropathy may be classified according to the number and distribution of nerves affected (mononeuropathy, mononeuritis multiplex, or polyneuropathy), the type of nerve cell predominantly affected (motor, sensory, autonomic), or the process affecting the nerves; e.g., inflammation (neuritis), compression (compression neuropathy), chemotherapy (chemotherapy-induced peripheral neuropathy).
Mononeuropathy
See also: Compression neuropathy and Ulnar neuropathy
Mononeuropathy is a type of neuropathy that only affects a single nerve.[5] Diagnostically, it is important to distinguish it from polyneuropathy because the fact that only one nerve is affected makes it more likely that the cause is a localized trauma or infection.
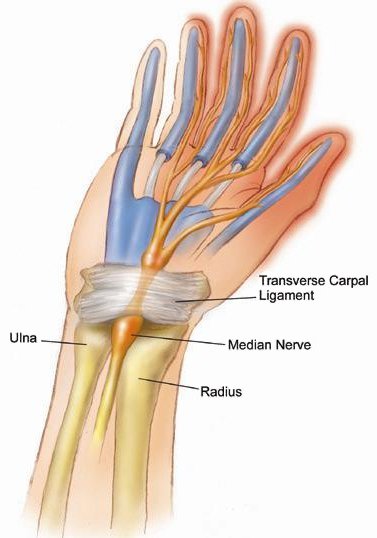
The most common cause of mononeuropathy is physical compression of the nerve, known as compression neuropathy. Carpal tunnel syndrome and axillary nerve palsy are examples of this. The "pins-and-needles" sensation of one's "foot falling asleep" (paresthesia) is caused by a compression mononeuropathy,[citation needed] albeit a temporary one that may be resolved merely by moving around and adjusting to a more appropriate position. Direct injury to a nerve, interruption of its blood supply (ischemia), or inflammation also may cause mononeuropathy.
Mononeuritis multiplex
Mononeuritis multiplex, occasionally termed polyneuritis multiplex, is simultaneous or sequential involvement of individual noncontiguous nerve trunks, either partially or completely, evolving over days to years and typically presenting with acute or subacute loss of sensory and motor function of individual nerves. The pattern of involvement is asymmetric, however, as the disease progresses, deficit(s) becomes more confluent and symmetrical, making it difficult to differentiate from polyneuropathy. Therefore, attention to the pattern of early symptoms is important.
Mononeuritis multiplex also may cause pain, which is characterized as deep, aching pain that is worse at night and frequently in the lower back, hip, or leg. In people with diabetes mellitus, mononeuritis multiplex typically is encountered as acute, unilateral, and severe thigh pain followed by anterior muscle weakness and loss of knee reflex.
Electrodiagnostic medicine studies will show multifocal sensory motor axonal neuropathy.
It is caused by, or associated with, several medical conditions:
- diabetes mellitus
- vasculitides: polyarteritis nodosa, granulomatosis with polyangiitis, and Churg–Strauss syndrome
- immune-mediated diseases, such as rheumatoid arthritis, lupus erythematosus (SLE)
- infections: leprosy, lyme disease, HIV
- sarcoidosis, amyloidosis
- cryoglobulinemia
- reactions to exposure to chemical agents, including trichloroethylene and dapsone
- rarely, following the sting of certain jellyfish, such as the sea nettle
Polyneuropathy
Main article: Polyneuropathy
Polyneuropathy is a pattern of nerve damage that is quite different from mononeuropathy, often more serious and affecting more areas of the body. The term "peripheral neuropathy" sometimes is used loosely to refer to polyneuropathy. In cases of polyneuropathy, many nerve cells in various parts of the body are affected, without regard to the nerve through which they pass; not all nerve cells are affected in any particular case. In distal axonopathy, one common pattern is that the cell bodies of neurons remain intact, but the axons are affected in proportion to their length. Diabetic neuropathy is the most common cause of this pattern. In demyelinating polyneuropathies, the myelin sheath around axons is damaged, which affects the ability of the axons to conduct electrical impulses. The third and least common pattern affects the cell bodies of neurones directly. This usually picks out either the motor neurones (known as motor neurone disease) or the sensory neurones (known as sensory neuronopathy or dorsal root ganglionopathy).
The effect of this is to cause symptoms in more than one part of the body, often symmetrically on left and right sides. As for any neuropathy, the chief symptoms include weakness or clumsiness of movement (motor); unusual or unpleasant sensations such as tingling or burning; reduction in the ability to feel texture, temperature, etc.; and impaired balance when standing or walking (sensory). In many polyneuropathies, these symptoms occur first and most severely in the feet. Autonomic symptoms also may occur, such as dizziness on standing up, erectile dysfunction, and difficulty controlling urination.
Polyneuropathies usually are caused by processes that affect the body as a whole. Diabetes and impaired glucose tolerance are the most common causes. Other causes relate to the particular type of polyneuropathy, and there are many different causes of each type, including inflammatory diseases such as lyme disease, vitamin deficiencies, blood disorders, and toxins (including alcohol and certain prescribed drugs).
Most types of polyneuropathy progress fairly slowly, over months or years, but rapidly progressive polyneuropathy also occurs. It is important to recognize that glucose levels in the blood may spike to nerve-damaging levels after eating even though fasting blood sugar levels and average blood glucose levels may still remain below normal levels (currently they typically are considered below 100 mg/dL for fasting blood plasma and 6.0% for HGBA1c, the test commonly used to measure average blood glucose levels over an extended period). Studies have shown that many of the cases of peripheral small fiber neuropathy with typical symptoms of tingling, pain, and loss of sensation in the feet and hands are due to glucose intolerance before a diagnosis of diabetes or pre-diabetes. Such damage often is reversible, particularly in the early stages, with changes in diet, exercise, and weight loss.
The treatment of polyneuropathies is aimed firstly at eliminating or controlling the cause, secondly at maintaining muscle strength and physical function, and thirdly at controlling symptoms such as neuropathic pain.
Autonomic neuropathy
Autonomic neuropathy is a form of polyneuropathy that affects the non-voluntary, non-sensory nervous system (i.e., the autonomic nervous system), affecting mostly the internal organs such as the bladder muscles, the cardiovascular system, the digestive tract, and the genital organs. These nerves are not under a person's conscious control and function automatically. Autonomic nerve fibers form large collections in the thorax, abdomen, and pelvis outside the spinal cord. They have connections with the spinal cord and ultimately the brain, however. Most commonly autonomic neuropathy is seen in persons with long-standing diabetes mellitus type 1 and 2. In most—but not all—cases, autonomic neuropathy occurs alongside other forms of neuropathy, such as sensory neuropathy.
Autonomic neuropathy is one cause of malfunction of the autonomic nervous system, but not the only one; some conditions affecting the brain or spinal cord also may cause autonomic dysfunction, such as multiple system atrophy, and therefore, may cause similar symptoms to autonomic neuropathy.
The signs and symptoms of autonomic neuropathy include the following:
- Urinary bladder conditions: bladder incontinence or urine retention
- Gastrointestinal tract: dysphagia, abdominal pain, nausea, vomiting, malabsorption, fecal incontinence, gastroparesis, diarrhoea, constipation
- Cardiovascular system: disturbances of heart rate (tachycardia, bradycardia), orthostatic hypotension, inadequate increase of heart rate on exertion
- Respiratory system: impairments in the signals associated with regulation of breathing and gas exchange (central sleep apnea, hypopnea, bradypnea).[6]
- Other areas: hypoglycemia unawareness, genital impotence, sweat disturbances
Neuritis
Neuritis is a general term for inflammation of a nerve[7] or the general inflammation of the peripheral nervous system. Symptoms depend on the nerves involved, but may include pain, paresthesia (pins-and-needles), paresis (weakness), hypoesthesia (numbness), anesthesia, paralysis, wasting, and disappearance of the reflexes.
Causes of neuritis include:
- Physical injury
- Infection
- Diphtheria
- Herpes zoster (shingles)
- Leprosy
- Lyme disease
- Chemical injury such as chemotherapy
- Radiation therapy
- Underlying conditions including: :
- Alcoholism
- Autoimmune disease, especially multiple sclerosis and Guillain-Barre syndrome
- Beriberi (vitamin B1 deficiency)
- Cancer
- Celiac disease[8]
- Diabetes (Diabetic neuropathy)
- Hypothyroidism
- Porphyria
- Vitamin B12 deficiency
- Vitamin B6 excess[9]
Types of neuritis include:
- Brachial neuritis
- Cranial neuritis such as Bell's palsy
- Optic neuritis
- Vestibular neuritis
- Wartenberg's migratory sensory neuropathy
Signs and symptoms
Those with diseases or dysfunctions of their nerves may present with problems in any of the normal nerve functions. Symptoms vary depending on the nerve fiber type that is involved.
In terms of sensory function, symptoms commonly include loss of function ("negative") symptoms, including numbness, tremor, impairment of balance, and gait abnormality.[10] Gain of function (positive) symptoms include tingling, pain, itching, crawling, and pins-and-needles. Motor symptoms include loss of function ("negative") symptoms of weakness, tiredness, muscle atrophy, and gait abnormalities; and gain of function ("positive") symptoms of cramps, and muscle twitch (fasciculations).[11]
In the most common form, length-dependent peripheral neuropathy, pain and parasthesia appears symmetrically and generally at the terminals of the longest nerves, which are in the lower legs and feet. Sensory symptoms generally develop before motor symptoms such as weakness. Length-dependent peripheral neuropathy symptoms make a slow ascent of leg, while symptoms may never appear in the upper limbs; if they do, it will be around the time that leg symptoms reach the knee.[12]
When the nerves of the autonomic nervous system are affected, symptoms may include constipation, dry mouth, difficulty urinating, and dizziness when standing.[11]
Diagnosis
Peripheral neuropathy may first be considered when an individual reports symptoms of numbness, tingling, and pain in feet. After ruling out a lesion in the central nervous system as a cause, diagnosis may be made on the basis of symptoms, laboratory and other testing, clinical history, and a detailed examination.
During physical examination, specifically a neurological examination, those with generalized peripheral neuropathies most commonly have distal sensory or motor and sensory loss, although those with a pathology (problem) of the nerves may be perfectly normal; may show proximal weakness, as in some inflammatory neuropathies, such as Guillain–Barré syndrome; or may show focal sensory disturbance or weakness, such as in mononeuropathies. Classically, ankle jerk reflex is absent in peripheral neuropathy.
A physical examination will involve testing the deep ankle reflex as well as examining the feet for any ulceration. For large fiber neuropathy, an exam will usually show an abnormally decreased sensation to vibration, which is tested with a 128-Hz tuning fork, and decreased sensation of light touch when touched by a nylon monofilament.[12]
Diagnostic tests include electromyography (EMG) and nerve conduction studies (NCSs), which assess large myelinated nerve fibers.[12] Testing for small-fiber peripheral neuropathies often relates to the autonomic nervous system function of small thinly- and un-myelinated fibers. These tests include a sweat test and a tilt table test. Diagnosis of small fiber involvement in peripheral neuropathy may also involve a skin biopsy in which a 3 mm-thick section of skin is removed from the calf by a punch biopsy, and is used to measure the skin intraepidermal nerve fiber density (IENFD)-- the density of nerves in the outer layer of the skin.[10] Reduced density of the small nerves in the epidermis supports a diagnosis of small-fiber peripheral neuropathy.
Laboratory tests include blood tests for vitamin B-12 levels, a complete blood count, measurement of thyroid stimulating hormone levels, a comprehensive metabolic panel screening for diabetes and pre-diabetes, and a serum immunofixation test, which tests for antibodies in the blood.[11]
Causes
The causes are grouped broadly as follows:
- Genetic diseases: Friedreich's ataxia, Charcot-Marie-Tooth disease,[13] hereditary neuropathy with liability to pressure palsy
- Metabolic and endocrine diseases: diabetes mellitus,[14] chronic renal failure, porphyria, amyloidosis, liver failure, hypothyroidism
- Toxic causes: drugs (vincristine, metronidazole, phenytoin, nitrofurantoin, isoniazid, ethyl alcohol, statins[15][16]), organic herbicides TCDD dioxin, organic metals, heavy metals, excess intake of vitamin B6 (pyridoxine). Peripheral neuropathies also may result from long term (more than 21 days) treatment with Linezolid (Zyvox).[citation needed]
- Adverse effects of fluoroquinolones: irreversible neuropathy is a serious adverse reaction of fluoroquinolone drugs[17]
- Inflammatory diseases: Guillain-Barré syndrome, systemic lupus erythematosus, leprosy, multiple sclerosis, Sjögren's syndrome, Babesiosis, Lyme disease, sarcoidosis,[18]
- Vitamin deficiency states: Vitamin B12 (Methylcobalamin), vitamin A, vitamin E, vitamin B1 (thiamin)
- Physical trauma: compression, pinching, cutting, projectile injuries (for example, gunshot wound), strokes including prolonged occlusion of blood flow, electric discharge, including lightning strikes
- Effect of chemotherapy - see Chemotherapy-induced peripheral neuropathy[19]
- Exposure to Agent Orange[20]
- Others: electric shock, HIV,[21] malignant disease, radiation, shingles
Treatment
The treatment of peripheral neuropathy varies based on the cause of the condition, and treating the underlying condition can aid in the management of neuropathy. When peripheral neuropathy results from diabetes mellitus or pre-diabetes, blood sugar management is key to treatment. In pre-diabetes in particular, strict blood sugar control can significantly alter the course of neuropathy.[10] In peripheral neuropathy that stems from immune-mediated diseases, the underlying condition is treated with intravenous immunoglobulin or steroids. When peripheral neuropathy results from vitamin deficiencies or other disorders, those are treated as well.[10]
Many treatment strategies for peripheral neuropathy are symptomatic.
A range of drugs that act on the central nervous system, such as drugs originally intended as antidepressants and antiepileptic drugs, have been found to be useful in managing neuropathic pain. Commonly used treatments include using a tricyclic antidepressant (such as amitriptyline) and antiepileptic therapies such as gabapentin or sodium valproate. These have the advantage that besides being effective in many cases, they are relatively low in cost. Voltanerv and Voltanerv 50 from Cogentrix Pharma in India is a novel combination of Pregabalin, Methylcobalamin and Alpha Lipoic Acid.
A great deal of research has been conducted between 2005 and 2010 resulting in indications that synthetic cannabinoids and inhaled cannabis are effective treatments for a range of neuropathic disorders.[22] Research has demonstrated that the synthetic oral cannabinoid Nabilone is an effective adjunct treatment option for neuropathic conditions, especially for people who are resistant, intolerant, or allergic to common medications.[23] Oral opiate derivatives were found to be more effective than cannabis for most people.[24] Smoked cannabis has been found to provide relief from HIV-associated sensory neuropathy.[25] Smoked cannabis also was found to relieve neuropathy associated with CRPS type I, spinal cord injury, peripheral neuropathy, and nerve injury.[26]
Pregabalin is an anticonvulsant drug used for neuropathic pain. It also has been found effective for generalized anxiety disorder. It was designed as a more potent successor to gabapentin, but is significantly more expensive, especially now that the patent on gabapentin has expired and gabapentin is available as a generic drug. Pregabalin is marketed by Pfizer under the trade name Lyrica.
Duloxetine, a serotonin-norepinephrine reuptake inhibitor, also is being used to reduce neuropathic pain.
Transcutaneous electrical nerve stimulation therapy may be effective and safe in the treatment of diabetic peripheral neuropathy. A recent review of three trials involving 78 patients found some improvement in pain scores after 4 and 6, but not 12 weeks of treatment and an overall improvement in neuropathic symptoms at 12 weeks.[27] A second review of four trials found significant improvement in pain and overall symptoms, with 38% of patients in one trial becoming asymptomatic. The treatment remains effective even after prolonged use, but symptoms return to baseline within a month of cessation of treatment.[28]
Neuropathy has been reported to make winter weather more perilous for older adults.[29] Often, people with neuropathy who live in areas with defined winters (such as the northern United States) report that their symptoms were much less severe after moving to places with an undefined winter, such as Florida or California.[citation needed]
Sometimes symptomatic relief for the pain of peripheral neuropathy is obtained by application of topical capsacin. Capsacin is the factor that causes heat in chili peppers. Relief up to 12 weeks is noted with high concentrations of capsacin applied cutaneously. Local anesthesia often is used to counteract the initial discomfort of the capsacin. More information is available in this review by the National Institute of Health.[30]
Some current research in animal models has shown that depleting neurotrophin-3 may oppose the demyelination present in some peripheral neuropathies by increasing myelin formation.[31]
References
- ^ a b c d Richard A C Hughes (23 February 2002). "Clinical review: Peripheral neuropathy". British Medical Journal 324: 466. doi:10.1136/bmj.324.7335.466.
- ^ a b c d Janet M. Torpy; Jennifer L. Kincaid; Richard M. Glass (21 April 2010). "Patient page: Peripheral neuropathy". Journal of the American Medical Association 303 (15). doi:10.1001/jama.303.15.1556.
- ^ a b c d "Peripheral neuropathy fact sheet". National Institute of Neurological Disorders and Stroke. 19 September 2012.
- ^ "neuropathy". Online Etymology Dictionary.
- ^ "Dorlands Medical Dictionary:mononeuropathy".
- ^ Vinik, AI; Erbas, T (2013). "Diabetic autonomic neuropathy.". Handbook of clinical neurology 117: 279–94. doi:10.1016/b978-0-444-53491-0.00022-5. PMID 24095132.
- ^ "neuritis" at Dorland's Medical Dictionary
- ^ Chin, RL; Latov, N (Jan 2005). "Peripheral Neuropathy and Celiac Disease.". Current treatment options in neurology 7 (1): 43–48. doi:10.1007/s11940-005-0005-3. PMID 15610706.
- ^ Rosenbloom, Mark; Tarabar, Asim; Adler, Robert A. "Vitamin Toxicity". Medscape Reference. Medscape. Retrieved 21 May 2013.
- ^ a b c d Cioroiu, Comana M.; Brannagan, Thomas H. (2014). "Peripheral Neuropathy". Current Geriatrics Reports 3 (2): 83–90. doi:10.1007/s13670-014-0079-4. ISSN 2196-7865.
- ^ a b c Azhary H, Farooq MU, Bhanushali M, Majid A, Kassab MY (2010). "Peripheral neuropathy: differential diagnosis and management". Am Fam Physician 81 (7): 887–92. PMID 20353146.
- ^ a b c Watson, James C.; Dyck, P. James B. (2015). "Peripheral Neuropathy: A Practical Approach to Diagnosis and Symptom Management". Mayo Clinic Proceedings 90 (7): 940–951. doi:10.1016/j.mayocp.2015.05.004. ISSN 0025-6196.
- ^ Gabriel JM, Erne B, Pareyson D, Sghirlanzoni A, Taroni F, Steck AJ (1997). "Gene dosage effects in hereditary peripheral neuropathy. Expression of peripheral myelin protein 22 in Charcot-Marie-Tooth disease type 1A and hereditary neuropathy with liability to pressure palsies nerve biopsies". Neurology 49 (6): 1635–40. doi:10.1212/WNL.49.6.1635. PMID 9409359.
- ^ Kiziltan ME, Akalin MA, Sahin R, Uluduz D (2007). "Peripheral neuropathy in patients with diabetes mellitus presenting as Bell's palsy". Neuroscience Letters 427 (3): 138–41. doi:10.1016/j.neulet.2007.09.029. PMID 17933462.
- ^ "Statin Drugs May Increase Risk Of Peripheral Neuropathy". ScienceDaily (St. Paul, Minnesota). 15 May 2002. Retrieved 21 May 2013.
- ^ "Statin Drugs May Increase Risk of Peripheral Neuropathy". AAN.com (Press release). St. Paul, Minnesota: American Academy of Neurology. 13 May 2002. Retrieved 21 May 2013.
- ^ Cohen, JS (December 2001). "Peripheral Neuropathy Associated with Fluoroquinolones" (PDF). Ann Pharmacother 35 (12): 1540–7. doi:10.1345/aph.1Z429. PMID 11793615.
- ^ Heck AW, Phillips LH 2nd (1989). "Sarcoidosis and the nervous system". Neurol Clin 7 (3): 641–54. PMID 2671639.
- ^ Wilkes, G (2007). "Peripheral neuropathy related to chemotherapy". Seminars in oncology nursing 23 (3): 162–73. doi:10.1016/j.soncn.2007.05.001. PMID 17693343.
- ^ "Service-Connected Disability Compensation For Exposure To Agent Orange" (PDF). Vietnam Veterans of America. April 2015. p. 4. Retrieved 20 August 2015.
- ^ Gonzalez-Duarte, A; Cikurel, K; Simpson, DM (2007). "Managing HIV peripheral neuropathy". Current HIV/AIDS reports 4 (3): 114–8. doi:10.1007/s11904-007-0017-6. PMID 17883996.
- ^ Hazekamp, Arno; Grotenhermen, Franjo (2010). "Review on clinical studies with cannabis and cannabinoids 2005-2009" (PDF). Cannabinoids (International Association for Cannabinoid Medicines) (5): 1–21. Retrieved 21 May 2013.
- ^ Skrabek RQ, Galimova L, Ethans K, Perry D (2008). "Nabilone for the treatment of pain in fibromyalgia". J. Pain 9 (2): 164–73. doi:10.1016/j.jpain.2007.09.002. PMID 17974490.
- ^ Frank B, Serpell MG, Hughes J, Matthews JN, Kapur D (2008). "Comparison of analgesic effects and patient toleration of nabilone and dihydrocodeine for chronic neuropathic pain: randomized, crossover, double blind study". BMJ 336 (7637): 119–201. doi:10.1136/bmj.39429.619653.80. PMC 2213874. PMID 18182416.
- ^ Abrams DI, Jay CA, Shade SB, Vizozo H, Reda H, Press S, Kelly ME, Rowbotham Mc, Petersen KL (2007). "Cannabis in painful HIV-associated sensory neuropathy: a randomized placebo-controlled trail". J. Neurology 68 (7): 515–21. doi:10.1212/01.wnl.0000253187.66183.9c. PMID 17296917.
- ^ Wilsey B, Marcotte T, Tsodikov A, Millman J, Bentley H, Gouaux B, Fishman S (2008). "A randomized, placebo-controlled, crossover trail of cannabis cigarettes in neuropathic pain". J. Pain 9 (6): 506–21. doi:10.1016/j.jpain.2007.12.010. PMID 18403272.
- ^ Jin DM, Xu Y, Geng DF, Yan TB (July 2010). "Effect of transcutaneous electrical nerve stimulation on symptomatic diabetic peripheral neuropathy: a meta-analysis of randomized controlled trials". Diabetes Res. Clin. Pract. 89 (1): 10–5. doi:10.1016/j.diabres.2010.03.021. PMID 20510476.
- ^ Pieber K, Herceg M, Paternostro-Sluga T (April 2010). "Electrotherapy for the treatment of painful diabetic peripheral neuropathy: a review". J Rehabil Med 42 (4): 289–95. doi:10.2340/16501977-0554. PMID 20461329.
- ^ Dillon, Helen (21 December 2009). "Neuropathy can make winter weather more perilous for older adults". All Things Aging. Retrieved 10 March 2012.
- ^ http://www.ncbi.nlm.nih.gov/pubmed/23450576
- ^ Liu N, Varma S, Tsao D, Shooter EM, Tolwani RJ (2007). "Depleting endogenous neurotrophin-3 enhances myelin formation in the Trembler-J mouse, a model of a peripheral neuropathy". J. Neurosci. Res. 85 (13): 2863–9. doi:10.1002/jnr.21388. PMID 17628499.
Further reading
- Latov, Norman (2007). Peripheral Neuropathy: When the Numbness, Weakness, and Pain Won't Stop. New York: American Academy of Neurology Press Demos Medical. ISBN 1-932603-59-X.
- Committee on Standards and Practice Parameters, American Society of Anesthesiologists (2000). "Practice advisory for the prevention of perioperative peripheral neuropathies: an updated report by the American Society of Anesthesiologists Task Force on prevention of perioperative peripheral neuropathies". Anesthesiology 92 (4): 1168–82. doi:10.1097/00000542-200004000-00036. PMID 10754638.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||
|
||||||||||||||
UpToDate Contents
全文を閲覧するには購読必要です。 To read the full text you will need to subscribe.
- 1. 下肢末梢神経症候群の概要 overview of lower extremity peripheral nerve syndromes
- 2. 上肢末梢神経症候群の概要 overview of upper extremity peripheral nerve syndromes
- 3. 外傷性単神経障害 traumatic mononeuropathies
- 4. 感覚消失患者へのアプローチ approach to the patient with sensory loss
- 5. 尿毒症性単神経障害 uremic mononeuropathy
English Journal
- Neurologic manifestations of lyme disease.
- Halperin JJ.SourceDepartment of Neurosciences, Overlook Hospital & Atlantic Health, 99 Beauvoir Avenue, Summit, NJ 07902, USA, john.halperin@atlantichealth.org.
- Current infectious disease reports.Curr Infect Dis Rep.2011 Aug;13(4):360-6.
- Borrelia burgdorferi infection, the tick-borne spirochetosis known as Lyme disease or Lyme borreliosis, involves the nervous system (neuroborreliosis) in 10% to 15% of patients. Common manifestations include lymphocytic meningitis, cranial neuritis, mononeuropathy multiplex, and painful radiculoneur
- PMID 21484219
- Mononeuropathy multiplex associated with acute parvovirus B19 infection: characteristics, treatment and outcome.
- Lenglet T, Haroche J, Schnuriger A, Maisonobe T, Viala K, Michel Y, Chelbi F, Grabli D, Seror P, Garbarg-Chenon A, Amoura Z, Bouche P.SourceDepartement de Neurologie, Hopital de la Pitie-Salpetriere, Assistance Publique des Hopitaux de Paris (APHP), 47-83 Boulevard de l'Hopital, 75651, Paris Cedex 13, France, timothee.lenglet@psl.aphp.fr.
- Journal of neurology.J Neurol.2011 Jul;258(7):1321-6. Epub 2011 Feb 2.
- To describe the characteristics of peripheral neuropathy related to acute parvovirus B19 (B19V) infection. We reviewed clinical, electrophysiological and histological data of three patients with peripheral neuropathy and positive B19V detection (IgG, IgM and PCR) compatible with acute infection. The
- PMID 21287183
Japanese Journal
- ステロイドパルス療法が多発単神経炎に対し有効であったChurg-Strauss症候群の1例 (特集 血管炎・血行障害)
- 澁谷 貴史,小松 成綱,高橋 一朗 [他]
- 皮膚科の臨床 53(2), 204-208, 2011-02
- NAID 40018707383
- 特発性血小板減少性紫斑病に関連した多発単神経障害の1例
- 中村 憲道,重藤 寛史,磯部 紀子,田中 正人,大八木 保政,吉良 潤一
- 臨床神経学 50(7), 482-484, 2010-07-01
- NAID 10026525703
Related Links
- Mononeuropathy is a type of neuropathy that only affects a single nerve. It is diagnostically useful to distinguish them from polyneuropathies, because the limitation in scope makes it more likely that the ...
Related Pictures





★リンクテーブル★
| リンク元 | 「モノニューロパチー」「mononeuritis」「単神経炎」 |
| 拡張検索 | 「mononeuropathy multiplex」「multiple mononeuropathy」 |
「モノニューロパチー」
- 英
- mononeuropathy
- 同
- 単発神経障害、単神経障害、単発神経炎、単神経炎
- 関
- 多発単神経炎、多発性単ニューロパチー症候群
単神経炎 : 約 75,200 件 単発神経炎 : 約 74 件 単神経障害 : 約 48,700 件 単発神経障害 : 約 195,000 件 モノニューロパチー : 約 571 件 単ニューロパチー : 約 3,200 件
「mononeuritis」
- 関
- mononeuritis multiplex、mononeuropathy、mononeuropathy multiplex、mononeuropathy multiplex syndrome