WordNet
- distort adversely; "Jealousy had jaundiced his judgment"
- yellowing of the skin and the whites of the eyes caused by an accumulation of bile pigment (bilirubin) in the blood; can be a symptom of gallstones or liver infection or anemia (同)icterus
- affect with, or as if with, jaundice
- showing or affected by prejudice or envy or distaste; "looked with a jaundiced eye on the growth of regimentation"; "takes a jaundiced view of societies and clubs"
- affected by jaundice which causes yellowing of skin etc (同)icteric, yellow
PrepTutorEJDIC
- 黄疸(おうだん) / ひがみ,ねたみ,偏見 / 〈人〉‘に'偏見をもたせる;〈見解など〉‘を'ゆがめる
- 黄疸にかかった / ひがんだ
Wikipedia preview
出典(authority):フリー百科事典『ウィキペディア(Wikipedia)』「2015/06/25 12:03:12」(JST)
wiki en
"Yellowing" redirects here. For the plant disease, see lethal yellowing. For paper degradation, see foxing. For the Charles Dickens character Jarndyce, see Jarndyce.
"icteric" redirects here. For the physiological event, see Ictal. For the songbird Icteria, see Yellow-breasted Chat.
|
Jaundice of the skin caused by hepatic failure
|
|
| ICD-10 | R17 |
|---|---|
| ICD-9 | 782.4 |
| DiseasesDB | 7038 |
| MedlinePlus | 003243 |
| MeSH | D007565 |
Jaundice (also known as icterus,[1] from the Greek word ίκτερος; adjectival form, icteric) is a yellowish pigmentation of the skin, the conjunctival membranes over the sclerae (whites of the eyes), and other mucous membranes caused by high blood bilirubin levels.[2] This hyperbilirubinemia subsequently causes increased levels of bilirubin in the extracellular fluid. Concentration of bilirubin in blood plasma is normally below 1.2 mg/dL (<25µmol/L). A concentration higher than approx. 3 mg/dL (>50µmol/L) leads to jaundice.[3] The term jaundice comes from the French word jaune, meaning yellow.
Jaundice is often seen in liver disease such as hepatitis or liver cancer. It may also indicate leptospirosis or obstruction of the biliary tract, for example by gallstones or pancreatic cancer, or less commonly be congenital in origin (e.g., biliary atresia).
Yellow discoloration of the skin, especially on the palms and the soles, but not of the sclera and mucous membranes (i.e. oral cavity) is due to carotenemia—a harmless condition[4] important to differentiate from jaundice.
Contents
- 1 Signs and symptoms
- 2 Differential diagnosis
- 2.1 Pre-hepatic
- 2.2 Hepatocellular
- 2.3 Post-hepatic
- 2.4 Neonatal jaundice
- 3 Pathophysiology
- 3.1 Hepatic events
- 4 Diagnostic approach
- 5 Complications
- 6 References
- 7 External links
Signs and symptoms
A 4-year-old boy with icteric (jaundiced) sclera which later proved to be a manifestation of hemolytic anemia due to G6PD deficiency following fava bean consumption.
The main symptom of jaundice is a the yellowish discoloration of the white area of the eye and the skin.
The conjunctiva of the eye are one of the first tissues to change color as bilirubin levels rise in jaundice. This is sometimes referred to as scleral icterus. However, the sclera themselves are not "icteric" (stained with bile pigment) but rather the conjunctival membranes that overlie them. The yellowing of the "white of the eye" is thus more properly termed conjunctival icterus. The term "icterus" itself is sometimes incorrectly used to refer to jaundice that is noted in the sclera of the eyes, however its more common and more correct meaning is entirely synonymous with jaundice.[1][5]
Differential diagnosis
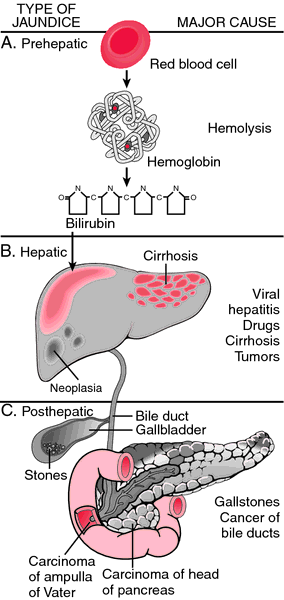
When a pathological process interferes with the normal functioning of the metabolism and excretion of bilirubin just described, jaundice may be the result. Jaundice is classified into three categories, depending on which part of the physiological mechanism the pathology affects. The three categories are:
Types of jaundice
| Category | Definition |
|---|---|
| Pre-hepatic/ hemolytic | The pathology is occurring prior to the liver due to
A.intrinsic defects in RB cells B. Extrinsic causes external to RB cells |
| Hepatic/ hepatocellular | The pathology is located within the liver caused due to disease of parenchymal cells of liver. |
| Post-Hepatic/ cholestatic | The pathology is located after the conjugation of bilirubin in the liver caused due to obstruction of biliary passage.[6] |
Pre-hepatic
Pre-hepaticular jaundice is caused by anything which causes an increased rate of hemolysis (breakdown of red blood cells). Unconjugated bilirubin comes from the breakdown of the heme pigment found in red blood cells' hemoglobin. The increased breakdown of red blood cells leads to an increase in the amount of unconjugated bilirubin present in the blood and deposition of this unconjugated bilirubin into various tissues can lead to a jaundiced appearance. In tropical countries, severe malaria can cause jaundice in this manner. Certain genetic diseases, such as sickle cell anemia, spherocytosis, thalassemia and glucose 6-phosphate dehydrogenase deficiency can lead to increased red cell lysis and therefore hemolytic jaundice. Commonly, diseases of the kidney, such as hemolytic uremic syndrome, can also lead to coloration. Defects in bilirubin metabolism also leads to jaundice, as in Gilbert's syndrome (a genetic disorder of bilirubin metabolism which can result in mild jaundice, which is found in about 5% of the population) and Crigler-Najjar syndrome, Type I and II.
In jaundice secondary to hemolysis, the increased production of bilirubin leads to the increased production of urine-urobilinogen. Bilirubin is not usually found in the urine because unconjugated bilirubin is not water-soluble, so, the combination of increased urine-urobilinogen with no bilirubin (since, unconjugated) in urine is suggestive of hemolytic jaundice.
Laboratory findings include:
- Urine: no bilirubin present, urobilinogen > 2 units (i.e., hemolytic anemia causes increased heme metabolism; exception: infants where gut flora has not developed).
- Serum: increased unconjugated bilirubin.
- Kernicterus is associated with increased unconjugated bilirubin; neonates are especially vulnerable to this due to increased permeability of the blood brain barrier.
Hepatocellular
Microscopy of cholestatic liver showing bilirubin pigment, H&E stain
Hepatocellular (hepatic) jaundice can be caused by acute or chronic hepatitis, hepatotoxicity, cirrhosis, drug-induced hepatitis and alcoholic liver disease. Cell necrosis reduces the liver's ability to metabolize and excrete bilirubin leading to a buildup of unconjugated bilirubin in the blood. Other causes include primary biliary cirrhosis leading to an increase in plasma conjugated bilirubin because there is impairment of excretion of conjugated bilirubin into the bile. The blood contains an abnormally raised amount of conjugated bilirubin and bile salts which are excreted in the urine. Jaundice seen in the newborn, known as neonatal jaundice, is common in newborns[7] as hepatic machinery for the conjugation and excretion of bilirubin does not fully mature until approximately two weeks of age. Rat fever (leptospirosis) can also cause hepatic jaundice. In hepatic jaundice, there is invariably cholestasis.
Laboratory findings depend on the cause of jaundice.
- Urine: Conjugated bilirubin present, urobilirubin > 2 units but variable (except in children). Kernicterus is a condition not associated with increased conjugated bilirubin.
- Plasma protein show characteristic changes.
- Plasma albumin level is low but plasma globulins are raised due to an increased formation of antibodies.
Bilirubin transport across the hepatocyte may be impaired at any point between the uptake of unconjugated bilirubin into the cell and transport of conjugated bilirubin into biliary canaliculi. In addition, swelling of cells and oedema due to inflammation cause mechanical obstruction of intrahepatic biliary tree. Hence in hepatocellular jaundice, concentration of both unconjugated and conjugated bilirubin rises in the blood. In hepatocellular disease, there is usually interference in all major steps of bilirubin metabolism—uptake, conjugation and excretion. However, excretion is the rate-limiting step, and usually impaired to the greatest extent. As a result, conjugated hyperbilirubinaemia predominates.[8]
The unconjugated bilirubin still enters the liver cells and becomes conjugated in the usual way. This conjugated bilirubin is then returned to the blood, probably by rupture of the congested bile canaliculi and direct emptying of the bile into the lymph leaving the liver. Thus, most of the bilirubin in the plasma becomes the conjugated type rather than the unconjugated type, and this conjugated bilirubin which did not go to intestine to become urobilinogen gives the urine the dark color.[9]
Post-hepatic
Post-hepatic jaundice, also called obstructive jaundice, is caused by an interruption to the drainage of bile containing conjugated bilirubin in the biliary system. The most common causes are gallstones in the common bile duct, and pancreatic cancer in the head of the pancreas. Also, a group of parasites known as "liver flukes" can live in the common bile duct, causing obstructive jaundice. Other causes include strictures of the common bile duct, biliary atresia, cholangiocarcinoma, pancreatitis, cholestasis of pregnancy, and pancreatic pseudocysts. A rare cause of obstructive jaundice is Mirizzi's syndrome.
In complete obstruction of the bile duct, no urobilinogen is found in the urine, since bilirubin has no access to the intestine and it is in the intestine that bilirubin gets converted to urobilinogen to be later released into the general circulation. In this case, presence of bilirubin (conjugated) in the urine without urine-urobilinogen suggests obstructive jaundice, either intra-hepatic or post-hepatic.
The presence of pale stools and dark urine suggests an obstructive or post-hepatic cause as normal feces get their color from bile pigments. However, although pale stools and dark urine are a feature of biliary obstruction, they can occur in many intra-hepatic illnesses and are therefore not a reliable clinical feature to distinguish obstruction from hepatic causes of jaundice.[10]
Patients also can present with elevated serum cholesterol, and often complain of severe itching or "pruritus" because of the deposition of bile salts.
No single test can differentiate between various classifications of jaundice. A combination of liver function tests is essential to arrive at a diagnosis.
| Function test | Pre-hepatic Jaundice | Hepatic Jaundice | Post-hepatic Jaundice |
|---|---|---|---|
| Total bilirubin | Normal / Increased | Increased | |
| Conjugated bilirubin | Normal | Increased | Increased |
| Unconjugated bilirubin | Normal / Increased | Increased | Normal |
| Urobilinogen | Normal / Increased | Decreased | Decreased / Negative |
| Urine Color | Normal | Dark (urobilinogen + conjugated bilirubin) | Dark (conjugated bilirubin) |
| Stool Color | Normal | Normal/Pale | Pale |
| Alkaline phosphatase levels | Normal | Increased | |
| Alanine transferase and Aspartate transferase levels | Increased | ||
| Conjugated Bilirubin in Urine | Not Present | Present | |
| Splenomegaly | Present | Present | Absent |
Neonatal jaundice
Main article: Neonatal jaundice
Neonatal jaundice is usually harmless: this condition is often seen in infants around the second day after birth, lasting until day 8 in normal births, or to around day 14 in premature births. Typical causes for neonatal jaundice include normal physiologic jaundice, jaundice due to formula supplementation,[12] and hemolytic disorders that include hereditary spherocytosis, glucose-6-phosphate dehydrogenase deficiency, pyruvate kinase deficiency, ABO/Rh blood type autoantibodies, or infantile pyknocytosis. Serum bilirubin normally drops to a low level without any intervention required. In cases where bilirubin rises higher, a brain-damaging condition known as kernicterus can occur, leading to significant disability.[2] This condition has been rising in recent years due to less time spent outdoors. A Bili light is often the tool used for early treatment, which often consists of exposing the baby to intensive phototherapy. Sunbathing is effective treatment,[13][14] and has the advantage of ultra-violet-B, which promotes Vitamin D production.[15] Bilirubin count is lowered through bowel movements and urination, so frequent and effective feedings are especially important.[16]
Pathophysiology
Jaundice itself is not a disease, but rather a sign of one of many possible underlying pathological processes that occur at some point along the normal physiological pathway of the metabolism of bilirubin in blood.
When red blood cells have completed their life span of approximately 120 days, or when they are damaged, their membranes become fragile and prone to rupture. As each red blood cell traverses through the reticuloendothelial system, its cell membrane ruptures when its membrane is fragile enough to allow this. Cellular contents, including hemoglobin, are subsequently released into the blood. The hemoglobin is phagocytosed by macrophages, and split into its heme and globin portions. The globin portion, a protein, is degraded into amino acids and plays no role in jaundice. Two reactions then take place with the heme molecule. The first oxidation reaction is catalyzed by the microsomal enzyme heme oxygenase and results in biliverdin (green color pigment), iron and carbon monoxide. The next step is the reduction of biliverdin to a yellow color tetrapyrol pigment called bilirubin by cytosolic enzyme biliverdin reductase. This bilirubin is "unconjugated," "free" or "indirect" bilirubin. Approximately 4 mg of bilirubin per kg of blood is produced each day.[17] The majority of this bilirubin comes from the breakdown of heme from expired red blood cells in the process just described. However approximately 20 percent comes from other heme sources, including ineffective erythropoiesis, and the breakdown of other heme-containing proteins, such as muscle myoglobin and cytochromes.[17]
Hepatic events
The unconjugated bilirubin then travels to the liver through the bloodstream. Because this bilirubin is not soluble, however, it is transported through the blood bound to serum albumin. Once it arrives at the liver, it is conjugated with glucuronic acid (to form bilirubin diglucuronide, or just "conjugated bilirubin") to become more water soluble. The reaction is catalyzed by the enzyme UDP-glucuronyl transferase.
This conjugated bilirubin is excreted from the liver into the biliary and cystic ducts as part of bile. Intestinal bacteria convert the bilirubin into urobilinogen. From here urobilinogen can take two pathways. It can either be further converted into stercobilinogen, which is then oxidized to stercobilin and passed out in the feces, or it can be reabsorbed by the intestinal cells, transported in the blood to the kidneys, and passed out in the urine as the oxidised product urobilin. Stercobilin and urobilin are the products responsible for the coloration of feces and urine, respectively.
Diagnostic approach
Biliary tract dilation due to obstruction as seen on CAT scan
Biliary tract dilation due to obstruction
Most patients presenting with jaundice will have various predictable patterns of liver panel abnormalities, though significant variation does exist. The typical liver panel will include blood levels of enzymes found primarily from the liver, such as the aminotransferases (ALT, AST), and alkaline phosphatase (ALP); bilirubin (which causes the jaundice); and protein levels, specifically, total protein and albumin. Other primary lab tests for liver function include gamma glutamyl transpeptidase (GGT) and prothrombin time (PT).
Some bone and heart disorders can lead to an increase in ALP and the aminotransferases, so the first step in differentiating these from liver problems is to compare the levels of GGT, which will only be elevated in liver-specific conditions. The second step is distinguishing from biliary (cholestatic) or liver (hepatic) causes of jaundice and altered laboratory results. The former typically indicates a surgical response, while the latter typically leans toward a medical response. ALP and GGT levels will typically rise with one pattern while aspartate aminotransferase (AST) and alanine aminotransferase (ALT) rise in a separate pattern. If the ALP (10–45 IU/L) and GGT (18–85) levels rise proportionately about as high as the AST (12–38 IU/L) and ALT (10–45 IU/L) levels, this indicates a cholestatic problem. On the other hand, if the AST and ALT rise is significantly higher than the ALP and GGT rise, this indicates an hepatic problem. Finally, distinguishing between hepatic causes of jaundice, comparing levels of AST and ALT can prove useful. AST levels will typically be higher than ALT. This remains the case in most hepatic disorders except for hepatitis (viral or hepatotoxic). Alcoholic liver damage may see fairly normal ALT levels, with AST 10x higher than ALT. On the other hand, if ALT is higher than AST, this is indicative of hepatitis. Levels of ALT and AST are not well correlated to the extent of liver damage, although rapid drops in these levels from very high levels can indicate severe necrosis. Low levels of albumin tend to indicate a chronic condition, while it is normal in hepatitis and cholestasis.
Lab results for liver panels are frequently compared by the magnitude of their differences, not the pure number, as well as by their ratios. The AST:ALT ratio can be a good indicator of whether the disorder is alcoholic liver damage (above 10), some other form of liver damage (above 1), or hepatitis (less than 1). Bilirubin levels greater than 10x normal could indicate neoplastic or intrahepatic cholestasis. Levels lower than this tend to indicate hepatocellular causes. AST levels greater than 15x tends to indicate acute hepatocellular damage. Less than this tend to indicate obstructive causes. ALP levels greater than 5x normal tend to indicate obstruction, while levels greater than 10x normal can indicate drug (toxic) induced cholestatic hepatitis or Cytomegalovirus. Both of these conditions can also have ALT and AST greater than 20× normal. GGT levels greater than 10x normal typically indicate cholestasis. Levels 5–10× tend to indicate viral hepatitis. Levels less than 5× normal tend to indicate drug toxicity. Acute hepatitis will typically have ALT and AST levels rising 20–30× normal (above 1000), and may remain significantly elevated for several weeks. Acetaminophen toxicity can result in ALT and AST levels greater than 50x normal.
Complications
Complications of jaundice include sepsis especially cholangitis, biliary cirrhosis, pancreatitis, coagulopathy, renal and liver failure. Other complications are related to the underlying disease and the procedures employed in the diagnosis and management of individual diseases. Cholangitis, especially the suppurative type (Charcot’s triad or Reynolds' pentad), is usually secondary to choledocholithiasis. It may also complicate procedures like ERCP. Treatment should include correction of coagulopathy, fluid/electrolyte anomaly, antibiotics and biliary drainage with ERCP where available or trans-hepatic drainage or surgery.
References
- ^ a b "Definition of Icterus". MedicineNet.com. 2011. Retrieved 3 February 2013.
- ^ a b Click, R; Dahl-Smith, J; Fowler, L; Dubose, J; Deneau-Saxton, M; Herbert, J (2013). "An osteopathic approach to reduction of readmissions for neonatal jaundice". Osteopathic Family Physician 5 (1): 17. doi:10.1016/j.osfp.2012.09.005.
- ^ Silbernagl S, Despopoulos A (2009). Color atlas of physiology (6 ed.). Thieme. p. 252. ISBN 978-3-13-545006-3.
- ^ Schwartz, Robert A. Carotenemia. emedicine.medscape.com
- ^ Icterus | Define Icterus at Dictionary.com. Dictionary.reference.com. Retrieved on 2013-12-23.
- ^ Shinde, MN Chatterjea, Rana (2012). Textbook of medical biochemistry (8 ed.). New Delhi: Jaypee Brothers Medical Publications (P) Ltd. p. 672. ISBN 9789350254844.
- ^ Collier J, Longore M, Turmezei T, Mafi AR (2010). "Neonatal jaundice". Oxford Handbook of Clinical Specialties. Oxford University Press. ISBN 978-0-19-922888-1.
- ^ Mathew K.G. (2008) Medicine: Prep Manual for Undergraduates, 3/e, Elsevier India, ISBN 8131211541, pp. 296–297
- ^ Hall, John Edward and Guyton, Arthur C. (2011) Textbook of Medical Physiology, Saunders/Elsevier, p. 841, ISBN 1416045740
- ^ Beckingham, IJ; Ryder, SD (2001). "Investigation of liver and biliary disease". BMJ (Clinical research ed.) 322 (7277): 33–6. doi:10.1136/bmj.322.7277.33. PMC 1119305. PMID 11141153.
- ^ Goljan, Edward F. (2007) Rapid Review Pathology, 2nd ed., Elsevier Health Sciences, pp. 368–369, ISBN 032304414X.
- ^ Bertini, G.; Dani, C.; Tronchin, M.; Rubaltelli, F. F. (2001). "Is breastfeeding really favoring early neonatal jaundice?". Pediatrics 107 (3): E41. doi:10.1542/peds.107.3.e41. PMID 11230622.
- ^ Sumida, K.; Kawana, M.; Kouno, E.; Itoh, T.; Takano, S.; Narawa, T.; Tukey, R. H.; Fujiwara, R. (2013). "Importance of UDP-glucuronosyltransferase 1A1 Expression in Skin and its Induction by Ultraviolet B in Neonatal Hyperbilirubinemia". Molecular Pharmacology 84 (5): 679–86. doi:10.1124/mol.113.088112. PMID 23950218.
- ^ Salih, F. M. (2001). "Can sunlight replace phototherapy units in the treatment of neonatal jaundice? An in vitro study". Photodermatology, photoimmunology & photomedicine 17 (6): 272–277. doi:10.1034/j.1600-0781.2001.170605.x. PMID 11722753.
- ^ Nakayama, J.; Imafuku, S.; Mori, T.; Sato, C. (2013). "Narrowband ultraviolet B irradiation increases the serum level of vitamin D3in patients with neurofibromatosis 1". The Journal of Dermatology 40 (10): 829–831. doi:10.1111/1346-8138.12256. PMID 23961975.
- ^ O'Keefe, Lori (May 2001). "Increased vigilance needed to prevent kernicterus in newborns". American Academy of Pediatrics 18 (5): 231.
- ^ a b Pashankar D, Schreiber RA (July 2001). "Jaundice in older children and adolescents". Pediatrics in Review 22 (7): 219–226. doi:10.1542/pir.22-7-219. PMID 11435623.
External links
- The dictionary definition of jaundice at Wiktionary
- Media related to Jaundice at Wikimedia Commons
|
||||||||||||||||||||||||||||||||||||||||||
|
UpToDate Contents
全文を閲覧するには購読必要です。 To read the full text you will need to subscribe.
- 1. 肝酵素および肝機能検査値の異常が認められた患者に対するアプローチ approach to the patient with abnormal liver biochemical and function tests
- 2. 妊娠性肝内胆汁うっ滞 intrahepatic cholestasis of pregnancy
- 3. 新生児や乳児の胆汁うっ滞への評価アプローチ approach to evaluation of cholestasis in neonates and young infants
- 4. 新生児や乳児に生じる胆汁うっ滞の原因 causes of cholestasis in neonates and young infants
- 5. 胆汁うっ滞関連そう痒症 pruritus associated with cholestasis
English Journal
- Recent advances in autoimmune pancreatitis: type 1 and type 2.
- Kamisawa T, Chari ST, Lerch MM, Kim MH, Gress TM, Shimosegawa T.SourceDepartment of Internal Medicine, Tokyo Metropolitan Komagome Hospital, , Tokyo, Japan.
- Gut.Gut.2013 Sep;62(9):1373-80. doi: 10.1136/gutjnl-2012-304224. Epub 2013 Jun 8.
- Autoimmune pancreatitis (AIP) is a form of chronic pancreatitis characterised clinically by frequent presentation with obstructive jaundice, histologically by a lymphoplasmacytic infiltrate with fibrosis, and therapeutically by a dramatic response to steroids. When so defined, AIP can be sub-classif
- PMID 23749606
- Isolated hepatobiliary cryptococcosis manifesting as obstructive jaundice in an immunocompetent child: case report and review of the literature.
- Zhang C, Du L, Cai W, Wu Y, Lv F.SourceDepartment of Pediatric Surgery, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, No. 1665, Kongjiang Road, Shanghai, 200092, China.
- European journal of pediatrics.Eur J Pediatr.2013 Aug 14. [Epub ahead of print]
- The majority of patients with symptomatic cryptococcosis have an underlying immunocompromising condition. In the absence of coexisting immunocompromising condition, Cryptococcus neoformans is rarely considered in the differential diagnosis of obstructive jaundice that occurs in children with hilar m
- PMID 23942746
Japanese Journal
- パクリタキセルの用量調節でTC療法後の肝障害増悪を回避しdose-dense化学療法を完遂できた卵巣がんの1例
- 医療薬学 41(2), 93-97, 2015
- NAID 130005125780
- 肝内胆汁うっ滞が遷延し急速な線維化の進行をともなうFCH様の病理所見を呈したC型急性肝炎の1例
- 日本消化機病學會雜誌. 乙 111(6), 1141-1148, 2014
- NAID 130004776838
Related Links
- Pruritus is the primary symptom of cholestasis and is thought to be due to interactions of serum bile acids with opioidergic nerves. In fact, the mixed opioid agonist/antagonist Naltrexone is used to treat pruritus due to cholestasis. jaundice.
- jaundice /jaun·dice/ (jawn´dis) icterus; yellowness of the skin, scleras, mucous membranes, and excretions due to hyperbilirubinemia and deposition of bile pigments. acholuric jaundice jaundice without bilirubinemia, associated with elevated ...
Related Pictures



★リンクテーブル★
| リンク元 | 「胆汁鬱滞性黄疸」「胆汁うっ滞性黄疸」 |
| 関連記事 | 「cholestatic」「jaundiced」「jaundice」 |
「胆汁鬱滞性黄疸」
「胆汁うっ滞性黄疸」
「cholestatic」
- adj.
- 胆汁うっ滞性の
- ex.
- cholestatic hepatitis 胆汁うっ滞性肝炎
「jaundiced」
- 黄疸性の
- 関
- icteric
「jaundice」