Wikipedia preview
出典(authority):フリー百科事典『ウィキペディア(Wikipedia)』「2015/10/03 06:44:14」(JST)
wiki en
UpToDate Contents
全文を閲覧するには購読必要です。 To read the full text you will need to subscribe.
- 1. 本態性振戦の外科治療 surgical treatment of essential tremor
- 2. 頭蓋に対する定位手術的照射 stereotactic cranial radiosurgery
- 3. ジストニアの治療 treatment of dystonia
- 4. Symptomatic (secondary) myoclonus
- 5. 舞踏病の概要 overview of chorea
English Journal
- Thalamic Connectivity in Patients with Essential Tremor Treated with MR Imaging-guided Focused Ultrasound: In Vivo Fiber Tracking by Using Diffusion-Tensor MR Imaging.
- Wintermark M1, Huss DS, Shah BB, Tustison N, Druzgal TJ, Kassell N, Elias WJ.Author information 1From the Department of Radiology, Neuroradiology Division (M.W., N.T., T.J.D.), Department of Neurosurgery (D.S.H., N.K., W.J.E.), and Department of Neurology (B.B.S.), University of Virginia, 1215 Lee St, New Hospital, 1st Floor, Room 1011, Charlottesville, VA 22908-0170; and Department of Radiology, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland (M.W.).AbstractPurpose To use diffusion-tensor (DT) magnetic resonance (MR) imaging in patients with essential tremor who were treated with transcranial MR imaging-guided focused ultrasound lesion inducement to identify the structural connectivity of the ventralis intermedius nucleus of the thalamus and determine how DT imaging changes correlated with tremor changes after lesion inducement. Materials and Methods With institutional review board approval, and with prospective informed consent, 15 patients with medication-refractory essential tremor were enrolled in a HIPAA-compliant pilot study and were treated with transcranial MR imaging-guided focused ultrasound surgery targeting the ventralis intermedius nucleus of the thalamus contralateral to their dominant hand. Fourteen patients were ultimately included. DT MR imaging studies at 3.0 T were performed preoperatively and 24 hours, 1 week, 1 month, and 3 months after the procedure. Fractional anisotropy (FA) maps were calculated from the DT imaging data sets for all time points in all patients. Voxels where FA consistently decreased over time were identified, and FA change in these voxels was correlated with clinical changes in tremor over the same period by using Pearson correlation. Results Ipsilateral brain structures that showed prespecified negative correlation values of FA over time of -0.5 or less included the pre- and postcentral subcortical white matter in the hand knob area; the region of the corticospinal tract in the centrum semiovale, in the posterior limb of the internal capsule, and in the cerebral peduncle; the thalamus; the region of the red nucleus; the location of the central tegmental tract; and the region of the inferior olive. The contralateral middle cerebellar peduncle and bilateral portions of the superior vermis also showed persistent decrease in FA over time. There was strong correlation between decrease in FA and clinical improvement in hand tremor 3 months after lesion inducement (P < .001). Conclusion DT MR imaging after MR imaging-guided focused ultrasound thalamotomy depicts changes in specific brain structures. The magnitude of the DT imaging changes after thalamic lesion inducement correlates with the degree of clinical improvement in essential tremor. © RSNA, 2014.
- Radiology.Radiology.2014 Mar 9:132112. [Epub ahead of print]
- Purpose To use diffusion-tensor (DT) magnetic resonance (MR) imaging in patients with essential tremor who were treated with transcranial MR imaging-guided focused ultrasound lesion inducement to identify the structural connectivity of the ventralis intermedius nucleus of the thalamus and determine
- PMID 24620914
- Structural changes in cerebellar outflow tracts after thalamotomy in essential tremor.
- Buijink AW1, Caan MW2, Contarino MF1, Schuurman PR3, van den Munckhof P3, de Bie RM4, Olabarriaga SD5, Speelman JD4, van Rootselaar AF6.Author information 1Department of Neurology and Clinical Neurophysiology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; Brain Imaging Center, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.2Brain Imaging Center, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; Department of Radiology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.3Department of Neurosurgery, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.4Department of Neurology and Clinical Neurophysiology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.5Department of Clinical Epidemiology, Biostatistics and Bioinformatics, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.6Department of Neurology and Clinical Neurophysiology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands; Brain Imaging Center, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands. Electronic address: a.f.vanrootselaar@amc.uva.nl.AbstractBACKGROUND: This study set out to determine whether structural changes are present outside the thalamus after thalamotomy in patients with essential tremor (ET), specifically in the cerebellorubrothalamic tracts. We hypothesized that diffusion tensor imaging (DTI) would detect these changes.
- Parkinsonism & related disorders.Parkinsonism Relat Disord.2014 Mar 5. pii: S1353-8020(14)00073-X. doi: 10.1016/j.parkreldis.2014.02.020. [Epub ahead of print]
- BACKGROUND: This study set out to determine whether structural changes are present outside the thalamus after thalamotomy in patients with essential tremor (ET), specifically in the cerebellorubrothalamic tracts. We hypothesized that diffusion tensor imaging (DTI) would detect these changes.METHODS:
- PMID 24637119
- Women pioneers in basal ganglia surgery.
- Hariz GM1, Rehncrona S2, Blomstedt P3, Limousin P4, Hamberg K5, Hariz M6.Author information 1Department of Clinical Neuroscience, Umeå University, Umeå, Sweden; Department of Community Medicine and Rehabilitation, Occupational Therapy, Umeå University, Umeå, Sweden.2Department of Neurosurgery, Lund University, Lund, Sweden.3Department of Clinical Neuroscience, Umeå University, Umeå, Sweden.4UCL Institute of Neurology, Queen Square, London, UK.5Department of Public Health and Clinical Medicine, Family Medicine, Umeå University, Umeå, Sweden.6Department of Clinical Neuroscience, Umeå University, Umeå, Sweden; UCL Institute of Neurology, Queen Square, London, UK. Electronic address: m.hariz@ucl.ac.uk.AbstractBACKGROUND: Stereotactic functional neurosurgery on basal ganglia has a long history and the pioneers are mostly men. We aimed at finding out if there were women who have contributed pioneering work in this field.
- Parkinsonism & related disorders.Parkinsonism Relat Disord.2014 Feb;20(2):137-41. doi: 10.1016/j.parkreldis.2013.11.002. Epub 2013 Nov 10.
- BACKGROUND: Stereotactic functional neurosurgery on basal ganglia has a long history and the pioneers are mostly men. We aimed at finding out if there were women who have contributed pioneering work in this field.METHODS: The literature was searched to identify women who have been first to publish i
- PMID 24262870
Japanese Journal
- パーキンソン病に対する外科治療
- 佐藤 澄人,隈部 俊宏
- 北里医学 = Kitasato medicine 43(2), 95-104, 2013-12
- NAID 40019954338
- パーキンソン病以外の運動機能異常症状に対する機能的外科治療の位置づけ
- 平 孝臣
- 臨床神経学 53(11), 966-968, 2013
- パーキンソン病や本態性振戦(ET)のような不随意運動疾患以外にも,重度の痙縮,運動麻痺回復などが外科治療の対象となる.ETではposterior subthalamic areaが新たなターゲットとして注目を浴びている.また低侵襲的治療としてMRI内でおこなう経頭蓋集束超音波照射治療が注目されている.全身性ジストニアでは淡蒼球内節のDBSが確立されている.書痙や音楽家の動作特異性局所ジストニアも視 …
- NAID 130004505484
- ジストニアの外科治療
- 平 孝臣
- 臨床神経学 52(11), 1077-1079, 2012
- … I have treated more than 100 patients with TSFHD with modern stereotactic thalamotomy of the nucleus ventro-oralis (Vo). … Stereotactic Vo thalamotomy is effective and safe for of task-specific focal hand dystonia. … Not only DBS but thalamotomy and other neurosurgical procedures play an important role in management of dystonias. …
- NAID 130004505063
Related Links
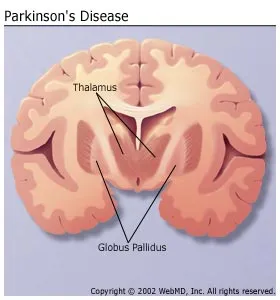
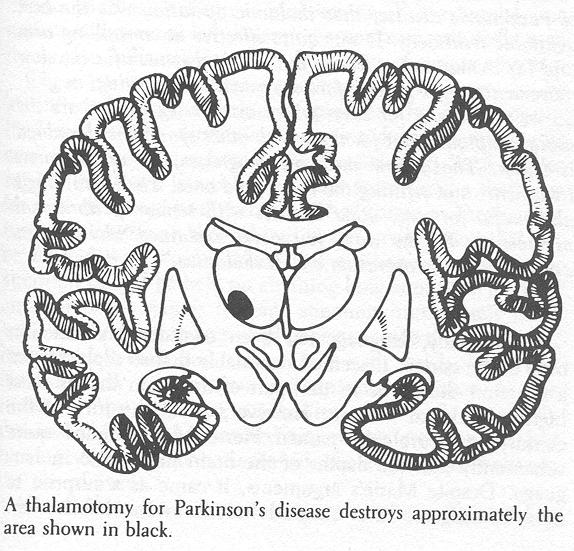
- thalamotomy [thal″ah-mot´ah-me] a stereotaxic surgical technique for the discrete destruction of specific groups of cells within the thalamus, as to relieve pain, to alleviate tremor and rigidity in parkinson's disease, or to relieve certain ...
- Thalamotomy is the precise destruction of a tiny area of the brain called the thalamus that controls some involuntary movements. ... Drugs & Supplements Get information and reviews on prescription drugs, over-the ...
Related Pictures



★リンクテーブル★
| リンク元 | 「視床手術」「視床破壊」 |
「視床手術」
- 英
- thalamotomy
- 関
- 視床破壊
「視床破壊」
- 英
- thalamotomy
- 関
- 視床手術