WordNet
- interrupt, break, or destroy; "fracture the balance of power"
- breaking of hard tissue such as bone; "it was a nasty fracture"; "the break seems to have been caused by a fall" (同)break
- fracture a bone of; "I broke my foot while playing hockey" (同)break
- become fractured; "The tibia fractured from the blow of the iron pipe"
- break (a bone); "She broke her clavicle"
- break into pieces; "The pothole fractured a bolt on the axle"
- violate or abuse; "This writer really fractures the language"
- the act of cracking something (同)crack, cracking
PrepTutorEJDIC
- 〈U〉(特に)骨を折ること;骨を折った状熊 / 〈C〉割れ(裂け)目,(鉱物の)破砕面 / 〈足・腕などを〉‘を'骨折する;…‘を'砕く / 骨折する;砕ける
Wikipedia preview
出典(authority):フリー百科事典『ウィキペディア(Wikipedia)』「2016/02/24 00:58:38」(JST)
wiki en
This article is about proximal femoral fractures. For fractures of the hip bone, see Pelvic fracture.
| Hip fracture | |
|---|---|
| Classification and external resources | |
|
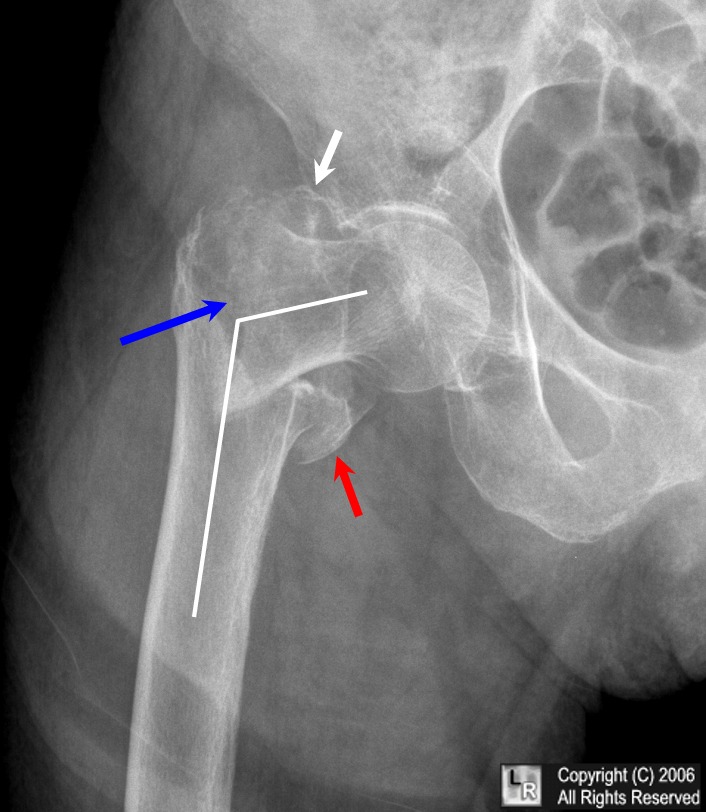
AP hip radiograph demonstrating an intertrochanteric fracture
|
|
| ICD-10 | S72.0 |
| AO | 31-A1 - 31-C3 |
| eMedicine | 825363 |
| MeSH | 68006620 |
A hip fracture is a serious femoral fracture[1] that occurs in the proximal end of the femur (the long bone running through the thigh), near the hip.
The term "hip fracture" is commonly used to refer to four different fracture patterns and is often due to osteoporosis; in the vast majority of cases, a hip fracture is a fragility fracture due to a fall or minor trauma in someone with weakened osteoporotic bone. Most hip fractures in people with normal bone are the result of high-energy trauma such as car accidents, falling from heights, or sports injuries.
In the UK, the mortality following a fractured neck of femur is between 20% and 35% within one year in people aged 82, ± 7 years, of whom 80% were women.[2]
Contents
- 1 Signs and symptoms
- 2 Risk factors
- 3 Mechanism
- 3.1 Functional Anatomy
- 3.2 Biomechanics
- 4 Diagnosis
- 4.1 Types
- 5 Prevention
- 6 Management
- 6.1 Intracapsular fractures
- 6.2 Intertrochanteric fracture
- 6.3 Subtrochanteric fractures
- 6.4 Rehabilitation
- 7 Complications
- 7.1 Surgical
- 7.2 Medical
- 8 Prognosis
- 8.1 Post operation
- 8.2 Canadian Collaborative Study of Hip Fractures
- 9 Epidemiology
- 9.1 Population
- 9.2 Age related
- 10 References
- 11 External links
Signs and symptoms
The classic clinical presentation of a hip fracture is an elderly patient who sustained a low-energy fall and now has pain and is unable to bear weight. On examination, the affected extremity is often shortened and unnaturally, externally rotated compared to the unaffected leg.
Risk factors
Hip fracture following a fall is likely to be a pathological fracture. The most common causes of weakness in bone are:
- Osteoporosis.
- Homocysteine, a toxic 'natural' amino acid linked to the cause of heart disease.
- Other metabolic bone diseases such as Paget's disease, osteomalacia, osteopetrosis and osteogenesis imperfecta. Stress fractures may occur in the hip region with metabolic bone disease.
- Benign or malignant primary bone tumours are rare causes of hip fractures.
- Metastatic cancer deposits in the proximal femur may weaken the bone and cause a pathological hip fracture.
- Infection in the bone is a rare cause of hip fracture.
- Smoking (associated with osteoporosis).
Mechanism
X-ray of the hip joint.
Functional Anatomy
The hip joint, an enarthrodial joint, can be described as a ball and socket joint. The femur connects at the acetabulum of the pelvis and projects laterally before angling medially and inferiorly to form the knee. Although this joint has three degrees of freedom, it is still stable due to the interaction of ligaments and cartilage. The labrum lines the circumference of the acetabulum to provide stability and shock absorption. Articular cartilage covers the concave area of acetabulum, providing more stability and shock absorption. Surrounding the entire joint itself is a capsule secured by the tendon of the psoas muscle and three ligaments. The iliofemoral, or Y, ligament is located anteriorly and serves to prevent hip hyperextension. The pubofemoral ligament is located anteriorly just underneath the iliofemoral ligament and serves primarily to resist abduction, extension, and some external rotation. Finally the ischiofemoral ligament on the posterior side of the capsule resists extension, adduction, and internal rotation. When considering the biomechanics of hip fractures, it is important to examine the mechanical loads the hip experiences during low energy falls.
Biomechanics
The hip joint is unique in that it experiences combined mechanical loads. An axial load along the shaft of the femur results in compressive stress. Bending load at the neck of the femur causes tensile stress along the upper part of the neck and compressive stress along the lower part of the neck. While osteoarthritis and osteoporosis are associated with bone fracture as we age, these diseases are not the cause of the fracture alone. In a study conducted in Umea, Sweden, Bergsten et al. discovered that low energy falls from heights of one meter or less were the leading cause of hip fracture in the elderly adult population [3] . Taking into account that falls were the leading cause of hip fracture, Hwang et al. studied how the manner in which a fall occurs affects the chances of hip fracture. In their study, they found three contributing factors, with fall direction being the strongest predictor.[4] During a sideways fall, the chances of hip fracture see a 15-fold and 12-fold increase in elderly males and females, respectively. This is likely due to a mechanical load experienced by bones weakened by osteoporosis.
Diagnosis
Intertrochanteric hip fracture in a 17-year-old male
Medial fracture in a 92-year-old woman
X-rays of the affected hip usually make the diagnosis obvious; AP (anteroposterior) and lateral views should be obtained.
In situations where a hip fracture is suspected but not obvious on x-ray, an MRI is the next test of choice. If an MRI is not available or the patient can not be placed into the scanner a CT may be used as a substitute. MRI sensitivity for radiographically occult fracture is greater than CT. Bone scan is another useful alternative however substantial drawbacks include decreased sensitivity, early false negative results, and decreased conspicuity of findings due to age related metabolic changes in the elderly.
As the patients most often require an operation, full pre-operative general investigation is required. This would normally include blood tests, ECG and chest x-ray.
Types
| Capsule | Area | Classification | ||
|---|---|---|---|---|
| Intracapsular | femoral head | AO 31-C1 - 31-C3 | Pipkin classification | |
| femoral neck | Subcapital | AO 31-B1 - 31-B3 | Garden classification, Pauwel's classification | |
| Transcervical | ||||
| Basicervical | ||||
| Extracapsular | Intertrochanteric | AO 31-A1 - 31-A3 | Evans' classification (1949), Ramadier's classification (1956), Boyd and Griffin's classification (1949), Decoulx & Lavarde's classification (1969), Ender's classification (1970), Tronzo's classification (1973), Evans-Jensen classification (1975), Deburge's classification (1976), Briot's classification (1980) | |
| Subtrochanteric | AO 32 | Seinsheimer classification | ||
Prevention
Hip protectors appear to decrease the number of hip fractures among the elderly.[5] They; however, are not often used.[5]
Management
Most hip fractures are treated by implanting an orthosis. The surgery is a major stress, particularly in the elderly. Pain is also significant, resulting in immobilization. Since prolonged immobilization can be more of a health risk than the surgery itself, post-op people are encouraged to become mobile as soon as possible, often with the assistance of physical therapy. Skeletal traction pending surgery is not supported by the evidence.[6] Regional nerve blocks are useful for pain management in hip fractures.[7]
Red blood cell transfusion is common for people undergoing hip fracture surgery due to the blood loss sustained during surgery and from the injury. Adverse effects of blood transfusion may occur and are avoided by restrictive use of blood transfusion rather than liberal use. Restrictive blood transfusion is based on symptoms of anemia and thresholds lower than the 10 g/dL haemoglobin used for liberal blood transfusion.[8]
If operative treatment is refused or the risks of surgery are considered to be too high the main emphasis of treatment is on pain relief. Skeletal traction may be considered for long term treatment. Aggressive chest physiotherapy is needed to reduce the risk of pneumonia and skilled rehabilitation and nursing to avoid pressure sores and DVT/pulmonary embolism Most people will be bedbound for several months. Non-operative treatment is no longer an alternative in developed countries with modern health care.[citation needed]
Intracapsular fractures
Fracture treated with cannulated screws
For low-grade fractures (Garden types 1 and 2), standard treatment is fixation of the fracture in situ with screws or a sliding screw/plate device. This treatment can also be offered for displaced fractures after the fracture has been reduced...
In elderly patients with displaced or intracapsular fractures many surgeons prefer to undertake a hemiarthroplasty, replacing the broken part of the bone with a metal implant. The advantage is that the patient can mobilize without having to wait for healing.
In elderly patients who are medically well and still active, a total hip replacement may be indicated.
Traction is contraindicated in femoral neck fractures due to it affecting blood flow to the head of the femur.[9]
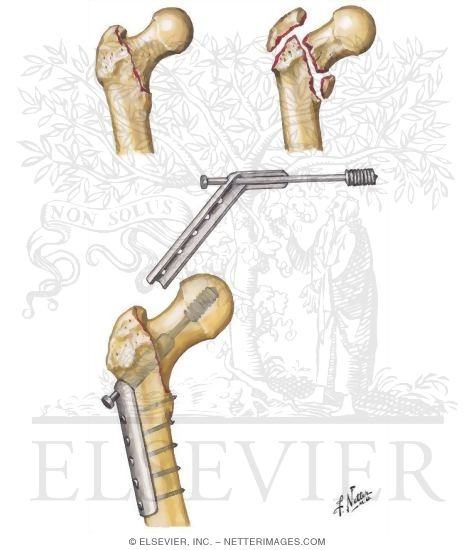
Intertrochanteric fracture
Fracture supported by dynamic hip screw
An intertrochanteric fracture, below the neck of the femur, has a good chance of healing. Treatment involves stabilizing the fracture with a lag screw and plate device to hold the two fragments in position. A large screw is inserted into the femoral head, crossing through the fracture; the plate runs down the shaft of the femur, with smaller screws securing it in place.
The fracture typically takes 3–6 months to heal. As it is only common in elderly, removal of the dynamic hip screw is usually not recommended to avoid unnecessary risk of second operation and the increased risk of re-fracture after implant removal. The most common cause for hip fractures in the elderly is osteoporosis; if this is the case, treatment of the osteoporosis can well reduce the risk of further fracture. Only young patients tend to consider having it removed; the implant may function as a stress riser, increasing the risk of a break if another accident occurs.
Subtrochanteric fractures
Subtrochanteric fractures may be treated with an intramedullary nail or a screw-plate construction and may require traction pre-operatively, though this practice is uncommon. It is unclear if any specific type of nail results in different outcomes than any other type of nail.[10]
Rehabilitation
Rehabilitation has been proven to increase daily functional status. It is unclear if the use of anabolic steroids effects recovery.[11]
Complications
Nonunion, failure of the fracture to heal, is common (20%) in fractures of the neck of the femur, but much more rare with other types of hip fracture. The rate of nonunion is increased if the fracture is not treated surgically to immobilize the bone fragments.
Malunion, healing of the fracture in a distorted position, is very common. The thigh muscles tend to pull on the bone fragments, causing them to overlap and reunite incorrectly. Shortening, varus deformity, valgus deformity, and rotational malunion all occur often because the fracture may be unstable and collapse before it heals. This may not be as much of a concern in patients with limited independence and mobility.
Avascular necrosis of the femoral head occurs frequently (20%) in fractures of the neck of femur, because the blood supply is interrupted. It is rare after intertrochanteric fractures.
Hip fractures rarely result in neurological or vascular injury.
Surgical
Deep or superficial wound infection has an approximate incidence of 2%. It is a serious problem as superficial infection may lead to deep infection. This may cause infection of the healing bone and contamination of the implants. It is difficult to eliminate infection in the presence of metal foreign bodies such as implants. Bacteria inside the implants are inaccessible to the body's defence system and to antibiotics. The management is to attempt to suppress the infection with drainage and antibiotics until the bone is healed. Then the implant should be removed, following which the infection may clear up.
Implant failure may occur; the metal screws and plate can break, back out, or cut out superiorly and enter the joint. This occurs either through inaccurate implant placement or if the fixation does not hold in weak and brittle bone. In the event of failure, the surgery may be redone, or changed to a total hip replacement.
Mal-positioning: The fracture can be fixed and subsequently heal in an incorrect position; especially rotation. This may not be a severe problem or may require subsequent osteotomy surgery for correction.
Medical
Many people are unwell before breaking a hip; it is common for the break to have been caused by a fall due to some illness, especially in the elderly. Nevertheless, the stress of the injury, and a likely surgery, increases the risk of medical illness including heart attack, stroke, and chest infection.
Blood clots may result. Deep venous thrombosis (DVT) is when the blood in the leg veins clots and causes pain and swelling. This is very common after hip fracture as the circulation is stagnant and the blood is hypercoagulable as a response to injury. DVT can occur without causing symptoms. A pulmonary embolism (PE) occurs when clotted blood from a DVT comes loose from the leg veins and passes up to the lungs. Circulation to parts of the lungs are cut off which can be very dangerous. Fatal PE may have an incidence of 2% after hip fracture and may contribute to illness and mortality in other cases.
Mental confusion is extremely common following a hip fracture. It usually clears completely, but the disorienting experience of pain, immobility, loss of independence, moving to a strange place, surgery, and drugs combine to cause delirium or accentuate pre-existing dementia.
Urinary tract infection (UTI) can occur. Patients are immobilized and in bed for many days; they are frequently catheterised, commonly causing infection.
Prolonged immobilization and difficulty moving make it hard to avoid pressure sores on the sacrum and heels of patients with hip fractures. Whenever possible, early mobilization is advocated; otherwise, alternating pressure mattresses should be used.
References:[12][13][14]
Prognosis
Hip fractures are very dangerous episodes especially for elderly and frail patients. The risk of dying from the stress of the surgery and the injury in the first thirty days is about 10%. At one year after fracture this may reach 30%.[15] If the condition is untreated the pain and immobility imposed on the patient increase that risk. Problems such as pressure sores and chest infections are all increased by immobility. The prognosis of untreated hip fractures is very poor.
Post operation
Among those affected over the age of 65, 40% are transferred directly to long-term care facilities, long-term rehabilitation facilities, or nursing homes; most of those affected require some sort of living assistance from family or home-care providers. 50% permanently require walkers, canes, or crutches for mobility; all require some sort of mobility assistance throughout the healing process.
Among those affected over the age of 50, approximately 25% die within the next year due to complications such as blood clots (deep venous thrombosis, pulmonary embolism), infections, and pneumonia.[citation needed]
Patients with hip fractures are at high risk for future fractures including hip, wrist, shoulder, and spine. After treatment of the acute fracture, the risk of future fractures should be addressed. Currently, only 1 in 4 patients after a hip fracture receives treatment and work up for osteoporosis, the underlying cause of most of the fractures. Current treatment standards include the starting of a bisphosphonate to reduce future fracture risk by up to 50%.
Canadian Collaborative Study of Hip Fractures
The Canadian Collaborative Study of Hip Fractures[16][17] compares health outcomes among patients exposed to various wait times before hip fracture surgery. The study tests whether preoperative deaths were more frequent among patients 65 years of age or older who remained untreated for non-medical reasons after admission for hip fracture. The study also tests whether postoperative complications and ensuing in-hospital deaths were less frequent when surgery was performed early after admission.
Led by health services researcher Boris Sobolev and orthopedic trauma surgeon Pierre Guy, a group of investigators across Canada was awarded a Canadian Institutes for Health Research grant to examine if patients benefited from having hip fracture surgery within 48-hours of admission, the national benchmark adopted by Canada’s health ministers in 2005.[18] The study seeks to provide evidence for the changes in hospital care that are required to prioritize access to hip fracture surgery and to enable policymakers to identify which patients benefit most from accelerated access to the procedure. The significance of this research arises from the opportunity to supplement existing knowledge about the benefits of expeditious hip fracture surgery[19][20] with evidence from real-life care delivered to a large number of patients across the entire country. The study aims to improve understanding of the pathways linking waits and health outcomes through a comparison of two types of in-hospital deaths, those occurring before surgery and those occurring after surgical complications.[21] Finally the study will identify groups of patients who would benefit from accelerated access to the procedure in terms of fewer complications and deaths.
Epidemiology
Hip fractures are seen globally and are a serious concern at the individual and population level. By 2050 it is estimated that there will be 6 million cases of hip fractures worldwide.[22] One study published in 2001 found that in the US alone, 310,000 individuals were hospitalized due to hip fractures, which can account for 30% of Americans who were hospitalized that year.[23] Another study found that in 2011, femur neck fractures were among the most expensive conditions seen in US hospitals, with an aggregated cost of nearly $4.9 billion for 316,000 inpatient hospitalizations.[24] Falling, poor vision, weight and height are all seen as risk factors. Falling is one of the most common risk factors for hip fractures. Approximately 90% of hip fractures are attributed to falls from standing height.[25]
Given the high morbidity and mortality associated with hip fractures, and the cost to the health system, in England and Wales the National hip fracture database is a mandatory nationwide audit of care and treatment of all hip fractures.
Population
All populations experience hip fractures but numbers vary with race, gender, and age. Women suffer three times as many hip fractures as men.[26] In a lifetime, men have an estimated 6% risk whereas postmenopausal women have an estimated 14% risk of suffering a hip fracture.[27] These statistics provide insight over a lifespan and conclude that women are twice as likely to suffer a hip fracture. The overwhelming majority of hip fractures occur in white individuals while blacks and Hispanics have a lower rate of them. This may be due to their generally greater bone density and also because whites have longer overall lifespan and higher likelihood of reaching an advanced age where the risk of breaking a hip goes up.[27] Deprivation is also a key factor: in England it has been found that people in the poorest parts of the country are more likely to fracture a hip and less likely to recover well than those in the least deprived areas.[28]
Age related
Age is the most dominant factor in hip fracture injuries, with most cases occurring in people over 75. The increase of age is related to the increase of hip fractures incidences.[22] Falls are the most common cause of hip fractures, around 30-60% of older adults fall each year. This increases the risk for hip fracture and leads to the increase risk of death in older individuals, the rate of one year mortality is seen from 12-37%.[29] For those remaining patients who do not suffer from mortality, half of them need assistance and cannot live independently. Also, older adults sustain hip fractures because of osteoporosis, which is a degenerative disease due to age and decrease in bone mass. The average age for suffering a hip fracture is 77 years old for women and 72 years old for men.[30] This shows how closely age is related to hip fractures.
References
- ^ TheFreeDictionary > hip fracture Citing: McGraw-Hill Concise Dictionary of Modern Medicine. Copyright 2002
- ^ Goldacre MJ, Roberts SE, Yeates D (October 2002). "Mortality after admission to hospital with fractured neck of femur: database study". BMJ 325 (7369): 868–9. doi:10.1136/bmj.325.7369.868. PMC 129634. PMID 12386038.
- ^ Bergström U., Björnstig U., Stenlund H., Jonsson H., Svensson O. (2008). "Fracture mechanisms and fracture pattern in men and women aged 50 years and older: a study of a 12 year population-based injury register, Umea, Sweden". Osteoporosis International 19: 1267–1273. doi:10.1007/s00198-007-0549-z.
- ^ Hwang H. F., Lee H. D., Huang H. H., Chen C. Y., Lin M. R. (2011). "Fall mechanisms, bone strength, and hip fractures in elderly men and women in Taiwan". Osteoporosis International 22: 2385–2393. doi:10.1007/s00198-010-1446-4.
- ^ a b Santesso, N; Carrasco-Labra, A; Brignardello-Petersen, R (Mar 31, 2014). "Hip protectors for preventing hip fractures in older people.". The Cochrane database of systematic reviews 3: CD001255. doi:10.1002/14651858.CD001255.pub5. PMID 24687239.
- ^ Handoll, HH; Queally, JM; Parker, MJ (Dec 7, 2011). "Pre-operative traction for hip fractures in adults.". Cochrane database of systematic reviews (Online) (12): CD000168. doi:10.1002/14651858.CD000168.pub3. PMID 22161361.
- ^ Ritcey, B; Pageau, P; Woo, MY; Perry, JJ (2 September 2015). "Regional Nerve Blocks For Hip and Femoral Neck Fractures in the Emergency Department: A Systematic Review.". CJEM: 1–11. doi:10.1017/cem.2015.75. PMID 26330019.
- ^ Brunskill, SJ; Millette, SL; Shokoohi, A; Pulford, EC; Doree, C; Murphy, MF; Stanworth, S (21 April 2015). "Red blood cell transfusion for people undergoing hip fracture surgery.". The Cochrane database of systematic reviews 4: CD009699. PMID 25897628.
- ^ Tintinalli, Judith E. (2010). Emergency Medicine: A Comprehensive Study Guide (Emergency Medicine (Tintinalli)). New York: McGraw-Hill Companies. ISBN 0-07-148480-9.
- ^ Queally, JM; Harris, E; Handoll, HH; Parker, MJ (Sep 12, 2014). "Intramedullary nails for extracapsular hip fractures in adults.". The Cochrane database of systematic reviews 9: CD004961. doi:10.1002/14651858.CD004961.pub4. PMID 25212485.
- ^ Farooqi, V; van den Berg, ME; Cameron, ID; Crotty, M (Oct 6, 2014). "Anabolic steroids for rehabilitation after hip fracture in older people.". The Cochrane database of systematic reviews 10: CD008887. doi:10.1002/14651858.CD008887.pub2. PMID 25284341.
- ^ "Fractures of the Femoral Neck". Wheeless' Textbook of Orthopaedics. Duke University School of Medicine. Retrieved 27 January 2008.
- ^ "Intertrochanteric Fractures". Wheeless' Textbook of Orthopaedics. Duke University School of Medicine. Retrieved 27 January 2008.
- ^ "Damage Control Orthopaedics: Patient Stabilization, Early Mobilization". 74th Annual Meeting of the American Academy of Orthopaedic Surgeons briefing. Medical News Today. 18 Feb 2007. Retrieved 27 January 2008.
- ^ Sedlář M, Kvasnička J, Krška Z, Tománková T, Linhart A (12 February 2015). "Early and subacute inflammatory response and long-term survival after hip trauma and surgery". Archives Gerontol. Geriatr. 60 (3): 431–6. doi:10.1016/j.archger.2015.02.002. PMID 25704919.
- ^ Centre for Hip Health and Mobility, Vancouver Coastal Health Research Institute. "48-Hour Benchmark for Hip Fracture Surgery for Older Adults".
- ^ Centre for Clinical Epidemiology and Evaluation, Vancouver Coastal Health Research Institute. "Evaluating the 48-hour Benchmark for Surgery: The Canadian Collaborative Study of Hip Fractures". c2e2.ca. Retrieved 2016-02-11.
- ^ Canadian Institute for Health Information. "Health Indicators 2007" (PDF).
- ^ McGuire, Kevin J.; Bernstein, Joseph; Polsky, Daniel; Silber, Jeffrey H. (2004-11-01). "The 2004 Marshall Urist award: delays until surgery after hip fracture increases mortality". Clinical Orthopaedics and Related Research (428): 294–301. ISSN 0009-921X. PMID 15534555.
- ^ Gdalevich, Michael; Cohen, Dani; Yosef, Dina; Tauber, Chanan (2004-06-01). "Morbidity and mortality after hip fracture: the impact of operative delay". Archives of Orthopaedic and Trauma Surgery 124 (5): 334–340. doi:10.1007/s00402-004-0662-9. ISSN 0936-8051. PMID 15095097.
- ^ Sheehan, Katie J.; Sobolev, Boris; Guy, Pierre; Bohm, Eric; Hellsten, Erik; Sutherland, Jason M.; Kuramoto, Lisa; Jaglal, Susan; Canadian Collaborative Study on Hip Fractures (2016-02-01). "Constructing an episode of care from acute hospitalization records for studying effects of timing of hip fracture surgery". Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society 34 (2): 197–204. doi:10.1002/jor.22997. ISSN 1554-527X. PMID 26228250.
- ^ a b Kannus P, Parkkari J, Sievanen H, Heinonen A, Vouri I, Jarvinen M (1996). "Epidemology of hip fractures". Bone 18: 57–63. doi:10.1016/8756-3282(95)00381-9.
- ^ Huddleston JM, Whitford KJ (2001). "Medical Care of Elderly Patients with Hip Fractures". Mayo Clinic Proceedings 76: 295–300. doi:10.4065/76.3.295.
- ^ Torio CM, Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. HCUP Statistical Brief #160. Agency for Healthcare Research and Quality, Rockville, MD. August 2013. [1]
- ^ Cumming RG, Nevitt MC, Cummings SR (1997). "Epidemiology of Hip Fractures". Epidemiology review 19 (2): 244–257. doi:10.1093/oxfordjournals.epirev.a017956.
- ^ "Hip Fractures Among Older Adults". CDC. CDC. Retrieved 13 May 2015.
- ^ a b Lauritzen JB (1997). "Hip fractures: Epidemiology, risk factors, falls, energy absorption, hip protectors, and prevention". Dan Med Bull 44 (2): 155–168.
- ^ Bardsley, Martin. "Focus on: Hip fracture". QualityWatch. Nuffield Trust & Health Foundation. Retrieved 13 May 2015.
- ^ Rubenstein LZ, Josephson KR (2002). "The Epidemiology of Falls and Syncope". Clinic in Geriatrics Medicine 18: 141–150.
- ^ Baumgaertner MR, Higgins TF. (2002) Femoral Neck Fractures. Rockwood & Green’s Fractures in Adults. 1579-1586
External links
| Wikimedia Commons has media related to Hip fractures. |
- Orthopedics.com article on hip fractures
- Fractures of the Femoral Neck Wheeless Textbook of Orthopaedics
- Intertrochanteric Fractures Wheeless' Textbook of Orthopaedics
- National Hip Fracture Database National Hip Fracture Database
- Proximal femoral fracture Musculoskeletal Radiology of Fractures
- National Osteoporosis Society National Osteoporosis Society
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
UpToDate Contents
全文を閲覧するには購読必要です。 To read the full text you will need to subscribe.
- 1. 成人における股関節骨折 hip fractures in adults
- 2. 成人における股関節痛の放射線評価 radiologic evaluation of the painful hip in adults
English Journal
- Use of administrative data for national surveillance of osteoporosis and related fractures in Canada: results from a feasibility study.
- O'Donnell S; Canadian Chronic Disease Surveillance System (CCDSS) Osteoporosis Working Group.Collaborators (15)Brown J, Jaglal S, Jean S, Leslie WD, Lix LM, McCrea P, McCrea L, Morin S, O'Donnell S, Onysko J, Papaioannou A, Reimer K, Rochette L, Siminoski K, Svenson L.
- Archives of osteoporosis.Arch Osteoporos.2013 Dec;8(1-2):143. doi: 10.1007/s11657-013-0143-2. Epub 2013 Jun 6.
- Using administrative data healthcare databases from five Canadian provinces, we compared prevalence estimates of diagnosed osteoporosis and incidence rates for related fractures in Canada. The algorithms adopted showed consistent age and sex patterns across all provinces and will be suitable for nat
- PMID 23740086
- Femur neck bone mineral density and fracture risk by age, sex, and race or Hispanic origin in older US adults from NHANES III.
- Looker AC.SourceNational Center for Health Statistics, Centers for Disease Control and Prevention, Room 4310 3311 Toledo Rd, Hyattsville, MD 2078, USA. ALooker@cdc.gov
- Archives of osteoporosis.Arch Osteoporos.2013 Dec;8(1-2):141. doi: 10.1007/s11657-013-0141-4. Epub 2013 May 29.
- Differences in the relationship between femur neck bone mineral density (FNBMD) and fracture risk were examined by age, sex, and race/ethnicity in the third National Health and Nutrition Examination Survey (NHANES III) cohort. FNBMD had similar, significant predictive utility for fracture in the dif
- PMID 23715737
- Incidence of hip fractures in Germany, 1995-2010.
- Icks A, Arend W, Becker C, Rapp K, Jungbluth P, Haastert B.SourceDepartment of Public Health, Faculty of Medicine, Heinrich-Heine University Düsseldorf, Moorenstr. 59, 40225 Düsseldorf, Germany. andrea.icks@uni-duesseldorf.de
- Archives of osteoporosis.Arch Osteoporos.2013 Dec;8(1-2):140. doi: 10.1007/s11657-013-0140-5. Epub 2013 May 15.
- We analyzed hip fracture incidence trends in Germany in 1995-2010, using national hospital discharge register. Overall, after age-sex-region adjustment, there was no significant trend. However, stratified analyses showed a significant decrease in younger people. In the elderly, there was a moderate
- PMID 23674147
Japanese Journal
- 症例 大腿骨転子部骨折治癒後に骨頭下骨折を来した2例
- 藤本 和弘,越智 康博,木戸 健司
- 日本職業・災害医学会会誌 = Japanese journal of occupational medicine and traumatology 62(4), 271-275, 2014-07
- NAID 40020171320
- 経験と考察 大腿骨転子部骨折AO分類31-A1,A2における遠位横止めを行わないlong nailの使用経験
- 松本 卓二,西山 大介,寺口 真年 [他]
- 整形外科 = Orthopedic surgery 65(2), 117-120, 2014-02
- NAID 40019955846
- 転倒により大腿骨転子部骨折を呈した症例 : 股関節外転筋筋力増強に関する一考察 (柳川リハビリテーション学院・福岡国際医療福祉学院症例研究発表会最優秀賞)
- 吉村 剛
- 柳川リハビリテーション学院・福岡国際医療福祉学院紀要 10, 64-66, 2014
- NAID 40020245168
Related Pictures




★リンクテーブル★
| リンク元 | 「転子間骨折」「trochanteric fracture」 |
| 関連記事 | 「fracture」 |
「転子間骨折」
「trochanteric fracture」
「fracture」
- n.